

Abstracts
Abstract
The pre-eminent figure in mid-Victorian psychological medicine, Dr. John Conolly had his reputation damaged in the 1850s by scandals linking him to cases of wrongful confinement, including one that figures in Charles Reade’s novel, Hard Cash. This essay looks at two major works Conolly published during the scandals and argues that they are responses to the charges against him. Both works focus on representations of insanity in art, rather than actual patients. “The Physiognomy of Insanity” (1858-59) is a series of essays on photographic portraits of asylum patients, and his essays prove to be more fictional than factual. A Study of Hamlet (1863) looks at the ambiguity of madness in Shakespeare’s portrayal of Hamlet, but it explains how Conolly understood the relationship between fact and fiction in cases of insanity. In both works, Conolly defends himself as an aesthete and defines his diagnostic method as a deliberate and necessary form of impressionism.
Article body
Charles Reade's 1863 novel, Hard Cash, dramatized the ease with which sane people could be confined to private lunatic asylums. This was a topical issue then, following the second of three "lunacy panics" in the nineteenth century: 1829-30, 1858-59, and 1876-77, and Reade’s was not the only novel to address the popular fear.[1] The protagonist—young, upright, Oxford-educated Alfred Hardie—is wrongfully confined to an asylum by his father, who has swindled him out of an inheritance. There, he develops a friendship, of sorts, with Dr. Wycherley, the asylum superintendent, who feels their elite education gives them something in common. Their conversations frequently turn to arts and letters, but most often it touches on Shakespeare:
in their midnight discussions, Dr. Wycherley more than once alluded to the insanity of Hamlet; and offered proofs. But Alfred declined the subject as too puerile. "A man must exist before he can be insane," said the Oxonian philosopher, severe in youthful gravity.
439; ch. 40
The topic is unusually important to the doctor, and he cannot bear to be contradicted on it—in this instance he falls into a teeth-grinding, foaming-at-the-mouth, "epileptic fit," from which Alfred discovers Wycherley's secret: he is a monomaniac fixated on Hamlet (440; ch. 40).
The statement that a "man must exist before he can be insane" is typical Charles Reade: a blunt, dismissive claim appealing to common sense.[2] He faults the doctor for confusing a fictional creation with a real person; however, it is not at all clear, in fact, that a man must exist before he can be insane. The statement is not only an ontological one but an epistemological claim referring to the inability of representation to capture the essence of insanity; in Hardie’s view, fictionalized insanity is a caricature that must always fall short of the original, and thus he dismisses the question outright. The description of Wycherley’s reaction exemplifies the problem, reducing insanity to a sketch of broad, recognizable strokes, like foaming at the mouth or falling into a fit. No ambiguity here. In Reade’s criticism of the asylum, the difference between insanity and its copy is self-evident.
Signs of insanity were considerably more problematic in the literature of nineteenth-century psychological medicine. There were few, if any, certain proofs of madness, and particularly vexing was the need to differentiate actual insanity from its imitation.[3] Physicians were well aware that some patients would create fictions designed to be accepted as facts; as John Haslam pointed out, one would fake the signs of insanity, while another would mask signs of the real thing (322). Diagnoses of insanity were frequently disputed in the medico-juridical setting on precisely these grounds, where a defendant might fake insanity to stay out of jail or fake sanity to avoid staying in a lunatic asylum. How was the specialist in insanity to differentiate real symptoms from signs that might be feigned?
The problem at issue here is representation. Can insanity be successfully imitated or reproduced, and, if so, what follows for the physician’s diagnostic procedures? The simplest solution is to obviate the problem by arguing that insanity cannot be reproduced, as Reade’s hero does. But nineteenth-century medical literature acknowledged, in both its content and its form, that it could. Medical books began to reproduce the visual signs of madness in their own pages. Beginning with Philippe Pinel’s Medico-Philosophical Treatise on Mental Alienation, or Mania (1801), technical illustrations appeared in medical books identifying types of insanity by their physical appearances, a development that followed directly from Lavater’s popularization of physiognomy in the 1770s.[4] By including illustrations, Esquirol’s Maladies Mentales (1838) and Alexander Morrison’s The Physiognomy of Mental Diseases (1838) assumed that the signs of insanity could be reproduced and that copies could contain the essence of mania and melancholia. Thus, when the imaginary Dr. Wycherley insists that a fictional character can, in fact, be insane, his fictional views are not far off the historical mark.
Hard Cash is itself a fiction, of course, but Dr. Wycherley was not entirely imaginary. He was recognizable to Reade’s audience as one of the most prominent doctors in Victorian psychological medicine, John Conolly, whose name had figured in the 1858-59 lunacy panic. Some of Conolly’s most distinctive remarks on the question of imitating insanity appear in two works devoted to artistic representations of madness. The first was a series of thirteen essays from 1858-59 on the earliest known photographs of the insane in Britain. The second was A Study of Hamlet (1863), the work that led Reade to parody Conolly’s Bardomania in Hard Cash. Taken together as related commentaries on the problem of copying insanity, these two works demonstrate a paradoxical stance on the issue, with opposite attitudes toward representations in life and in art. Conolly argues that an experienced physician can sense the difference between patients with real or feigned insanity, even if he cannot explain precisely why, so that insanity cannot successfully be reproduced in life. However, imitation can succeed in aesthetic works, like photography or Hamlet or fiction, by minimizing literality and taking liberties with the real thing.
* * *
While Conolly was superintendent of Hanwell Asylum from 1834-40, he became the first English doctor to convert a large, public asylum to the system of non-restraint.[5] By eliminating the older chains and straitjackets, he became a revered public figure, representing the efficacy of humanitarian reform. His status was considerably altered twenty years later, when the first installment of Hard Cash appeared in Charles Dickens’s monthly, All the Year Round. Conolly was then semi-retired, still much in the public eye, and nursing a dubious reputation.[6] He had been involved in several cases of wrongful confinement that were widely reported in the London press. His involvement in the June 1858 commitment of novelist Rosina Bulwer Lytton was notorious.[7] She was abducted by force and confined to Wyke House, a private lunatic asylum, by her estranged husband, Edward Bulwer-Lytton. Unhappy with her activities—she had disrupted one of his political campaign appearances—he had sought Conolly's aid, presumably for a sizeable fee, and Conolly duly certified her insane. However, a public uproar soon turned the incident into a political liability for Bulwer-Lytton, so three weeks later Conolly dutifully uncertified her, saying she was cured. The incident left the distinct impression that Conolly was a psychiatric hired gun. As Rosina Lytton wrote in 1866, that "vile old Dr. Conolly [. . .] would sell his own mother [. . .] for money."[8] By then, such a view was not unusual.[9]
In an aside, Rosina Lytton asked if Conolly had not "published some rubbish about 'Hamlet'?" (88). And so he had. His Study of Hamlet appeared early in 1863, during the serialization of Hard Cash, and Reade incorporated it into later installments. He was by no means subtle in identifying Dr. Wycherley as Conolly. In other chapters, Wycherley repeats Conolly's testimony in a widely publicized 1859 civil trial for wrongful confinement, "Ruck v. Stilwell and Another," alias Conolly.[10] Mrs. Ruck suspected her husband of having two children with one Mary Jones, a relative of hers. She testified that, during a drinking binge, Ruck accused her of “general prostitution” and demonstrated other delusions, so she arranged with two doctors, including Conolly, to have him committed to Moorcroft Asylum, run by Conolly’s former assistant, Dr. Stillwell. [11] Ruck languished there for ten months. Conolly had testified previously, in a Commission in Lunacy that was covered daily in the Times, that he was "in no way connected" with the asylum, but in the trial it turned out that he was paid regularly for referrals to Moorcroft, to the tune of £800 per year, and he had in fact received a quarterly fee of 15% on Ruck’s boarding costs at the asylum.[12] He had also signed the certificate after inspecting Ruck in the presence of the second signatory, a practice specifically forbidden by the 1828 Madhouses Act, which required two independent diagnoses.[13] The jury “found that Dr. Conolly was the regular professional attendant, with 500l. damages.”[14] He could ill afford this money.[15] The incident was an embarrassment to a medical profession then struggling to assert its authority over all matters pertaining to insanity, including the exclusive right to certify insanity, and it led to a revision of the law further specifying what it meant to be "connected" with an asylum.[16] The Ruck trial helped to end Conolly's career by compromising his reputation; following it, he went into semi-retirement, where he continued his practice of writing articles for professional journals and finally found the time to begin dabbling at his Study of Hamlet.
The question of graft has largely overshadowed other problems posed by these trials, problems that have a much larger significance to mid-Victorian mental medicine than whether or not Conolly was a crook. The underlying question is epistemological: how are signs of insanity to be read? More particularly, how does the physician interpret the patient's externally observable signs—speech and behavior—in estimating the internal psychological state? Complicating the problem of interpretation was the lack of consensus in the nineteenth century on what qualified as insanity. Absent an accepted clear-cut definition—the kind you could point to in a book—medical witnesses in legal proceedings had difficulty convincing juries that a diagnosis of insanity was based on science and not on the subjective vagaries of the physician's imagination, or, as in Conolly's case, the physician's purse. The problems in definition were two-fold: there was thought to be a wide variety of behaviors among sane people, making it very difficult to isolate specific behaviors that signified insanity and not eccentricity.[17] Second, sanity and insanity were seen as shading into one another on a continuum, and it was almost impossible to argue with any degree of certainty where the dividing line lay between a barely sound mind and a slightly unsound one. Legal experts were convinced the problem was unsolvable, but physicians in medical jurisprudence literature kept trying. Haslam, for example, thought that an ability to perform simple mathematical calculations was critical. Others stressed a patient's ability to be instructed or their general knowledge of worldly affairs.
Definitions of insanity also changed during the century, and expert opinions changed with them. In 1830, Conolly defined insanity narrowly and specifically excluded eccentricity.[18] But by 1848, when he served as an expert witness in Nottidge v. Ripley, his views had changed so radically that he disputed a judge's ruling that quoted from Conolly’s own earlier definition.[19] At this point, he considered not only eccentricity but also socially inappropriate behaviors as important signs of insanity. His definition of insanity was certainly capacious, but no more so than that of his peers. Historically, the boundaries of insanity progressively encroached on the terrain of sanity throughout the nineteenth century. In 1832, John Haslam was the exception when he claimed he "never saw any human who was of sound mind” (qtd. in Scull, Most Solitary 350n52). Three years later, James Cowles Prichard published his Treatise on Insanity (1835), which initiated a new era in Victorian mental medicine with the invention of "Moral Insanity," a kind of partial insanity that accounted for socially unacceptable or unconventional behaviors. Prichard wrote:
In cases of this description the moral and active principles [. . .] are strangely perverted and depraved; the power of self-government is lost or greatly impaired; and the individual is found to be incapable, not of talking or reasoning upon any subject proposed to him [. . .] but of conducting himself with decency and propriety in the business of life.
qtd. in Taylor and Shuttleworth 252
Also known as “partial insanity” and related to “monomania,” moral insanity is melancholia or mania on a discrete topic. Otherwise, the mind is untouched and so the condition easily passes unnoticed. Certainly, the bodily signs were unobservable to most. Forbes Winslow pointed out that the physician might "discover the first scintillations of brain disease, even when the patient and those about him repudiate all idea of cerebral ill health, and refuse to acknowledge, the necessity for medical advice, or treatment," a tricky situation, indeed, when someone is being certified and confined against his or her will.[20] As moral insanity became accepted, ever-broader definitions of insanity appeared.
Problems in definition led to public disagreement among medical experts in Lunacy Commission proceedings as well as civil trials. In the Ruck Commission, for example, expert witnesses were called on both sides; half of them insisted Ruck was sane while the other half were equally certain he was insane.[21] The presiding judge noted in jury instructions that the opinions cancelled each other out, and all of this confusion was publicized in the Times and the other major papers that reported at length on each day of the five-day case.[22] Such incidents did not promote public confidence in the objectivity of specialists at the time.
* * *
The Ruck scandal was in progress as Conolly published his series of thirteen essays on "The Physiognomy of Insanity," in the Medical Times and Gazette (Jan. 2, 1858 to Feb. 19, 1859). These essays centered on the problem of recognizing insanity from physical appearances, and they were accompanied by full-page engravings based on photographic portraits of ten different asylum patients.[23] In his essays, he discusses the promise of photography to fill the medical profession's need for images that could, as he put it, "give the singular expression arising from morbid movements of the mind" ("Physiognomy 1" 3b). None existed, he argues, notwithstanding the engravings used by Esquirol and Morrison, and so photography offered the first real opportunity to train medical students to recognize cases of insanity without prior experience.[24]
Conolly specifically published the essays and engravings for an audience of medical professionals, as illustrations of the outward signs of mental disorder. Modern reprintings of these images have reinforced this diagnostic framing by reducing the text of his essays to the immediate analysis of the images, leaving out the additional remarks that generally constituted the better part of the essays.[25] Conolly's style—Henry Maudsley termed it "graceful but diffuse" (173)—does not lend itself well to this usage, which has led to misunderstandings about his position on the photographs, as well as on the broader objective of his essay series. In the most influential edition of Conolly’s essays, Sander Gilman argues that Conolly fell for the “fallacy that the photograph presented an objective portrayal of the mentally ill” (Face 12). Read in their entirety, however, the essays suggest that, rather than seeing the photographs as an unambivalent boon to medical science, he thought that their diagnostic value was severely limited. In the explanation of those limitations, he clarifies the premises of his own diagnostic method and illustrates that madness can never be understood through the study of objective signs alone. His method was under attack at the time in the Ruck scandal, so his essays give him a platform to reassert his professional integrity to his peers.
Conolly defines physiognomy as a subtle art, when considered as a register of insanity, and he is quick to correct erroneous assumptions: "physiognomy is not a mere matter of eyebrows, and noses, and chins, and ears" ("Physiognomy 10" 212a). It is instead the study of changing facial expressions, bodily postures, and movements. As he explains physiognomy’s underlying principles, the muscles of the face are controlled by nerves that connect them to the brain. Through an unknown process, mental states caused by the experiences of pleasure and pain are communicated to the facial muscles so that external expressions make the mind visible. He sums up the theory as follows: "We vainly attempt to say where these movements of the mind originate," but they "stamp their meaning in muscular changes productive of an external language as plain [in its meaning] as its origin is beyond man's comprehension" ("Physiognomy 10" 211a). That "language is legible," he clarifies, in the most delicate movements of the eyelid, in the “marvelous [. . .] expression of the eyes,” in bodily attitude, and in the “demonstrative” movements of the fingers and hands. To Conolly, physiognomy is a study of the “effect on the observer” of minute flickering expressions, “rapid mutations.” These are so subtle that even if one is “fixed by the photographer [. . .] it still almost defies analysis,” making it impossible to point to any definite cause of the impression, even when every viewer reacts in the same way ("Physiognomy 10" 211a).
Conolly sees the images that accompany his essays as deeply flawed. He acknowledges their strengths; they “produce copies of nature, possessing a truthfulness and preserving minutiae which could not easily be perpetuated by any of the old methods” ("Physiognomy 1" 3b). But he repeatedly complains about the inadequacy of photography as a medium for copying insanity: “Neither painter nor photographer can catch and fix the innumerable shadows passing over the human face, as rapid in succession, and as fleeting in their nature, as the thoughts evolved in the perhaps ever changing molecules of the brain” ("Physiognomy 9" 81b). Such “fugitive impressions" will always elude even "the most dextrous snatches of the sun-aided photographer himself" ("Physiognomy 9" 81b). Given this fundamental inadequacy, why would he agree to write these essays? In particular, why take the counter-intuitive step of producing a series of thirteen essays on the physiognomy of insanity illustrated not even by the imperfect photographs but by engravings of the photographs reproduced in newsprint—a copy of a copy of a copy of insanity? He is certainly aware of the deficiencies of the resulting images. His analyses include close readings of the portraits, pointing to minute details in the face, the brow, the attitude. In the face of “Religious Mania,” for example, he notes “the compression of the upper lip” (fig. 1; “Physiognomy 9” 83a). Other details in the portrait defy description, though they are, he insists, there: he identifies “traces of expression, but which words cannot distinctly express, in the upper portion of the cheeks” (“Physiognomy 9” 83a). Similarly, in “Religious Mania: Convalescence,” he finds “a gentle smile pervading the features, to which it would be in vain to attempt to assign any narrow locality” (fig. 2; “Physiognomy 10” 212a).
Figure 1
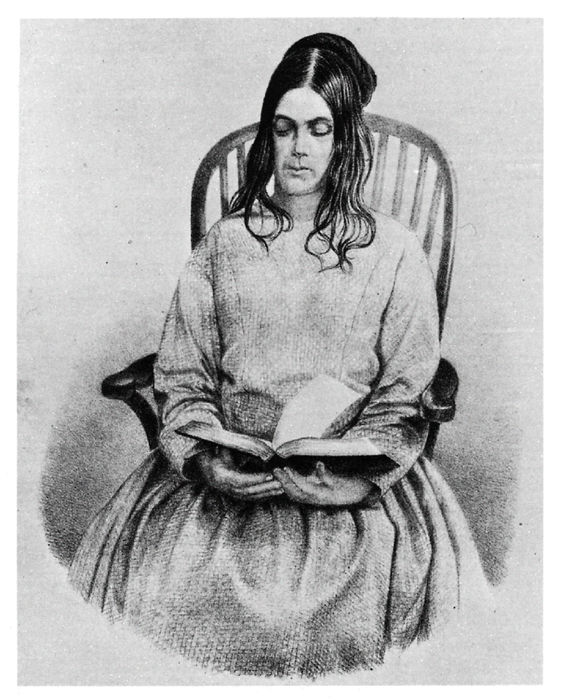
Plate 8, “Religious Mania”
Figure 2

Plate 9, “Religious Mania: Convalescence”
While such ineffable qualities pose one kind of problem, another is tangible inaccuracies in the reproductions. He regularly points to errors in the engravings, citing differences between them and the photographs that only he can actually see. Some are overt. “Religious Melancholia and Convalescence” is a before-and-after sequence. In the first image, she has self-inflicted scratches and scars on her face that are “not represented in the engraving” (fig. 3 left; “Physiognomy 11” 368b). Her hands are clenched, but these are cropped from the printed version. With such impediments to the basic project of illustrating the physiognomy of insanity, the entire attempt seems pointless if the images are, in fact, to be considered as diagnostically-useful documentary evidence.
Figure 3
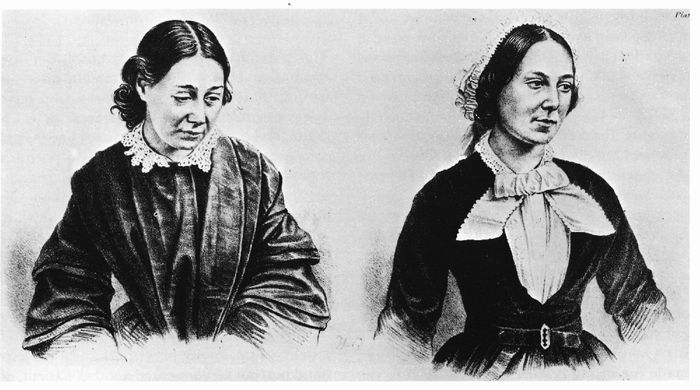
Plate 10, “Religious Melancholia and Convalescence”
The defining move in his recuperation of the photographs is also the one easiest to overlook—his decision not to identify the individuals portrayed, assigning them to a longstanding state of anonymity. His essays supply several details of the individual’s history, but case histories necessarily de-individualize the patient, who becomes a predominantly physical entity with a sketchy history. The case notes of the physicians at Bethlem at the time reflect this process, and they are considerably more detailed than the brief case notes for the county asylums.[26] In addition, anonymity was conventional for mental patients—insanity was a stigma with a taint of hereditary madness that few families could incur. In that respect, these essays were singular for the time; with the patient’s photographs reproduced as full-page engravings, patient anonymity was severely compromised, at best. While a moot issue, that anonymity is rhetorically useful to fix attention on the diagnostic label underneath the engraving. It substitutes for the person’s name, displacing the sign that identifies the patient as individual, and so divorces image from historical referent—that this is a particular person in a particular time and place and with a particular history. Without those details, the image becomes an unambivalent representation of an abstract disease model. The examples above are portraits of concepts, not individuals, named “Religious Mania” and “Religious Melancholia.”
This lack of status as historical documents also presents Conolly with an opportunity. Unmoored from their grounding in historical referentiality, they become more open to interpretation, and so the images can be made into anything that Conolly wants. If a detail is not clearly visible, he can assure us of its presence. Similarly, he is free to take liberties with the biographical details of the patient’s history; his readers have no way to judge the accuracy of his statements. An excellent essayist, Conolly only includes details that relate thematically to each essay’s argument. Ultimately, these essays and accompanying images belong more to the realm of fiction than fact, of art than science, and Conolly uses this freedom to redefine the portraits to suit his own purposes. To appreciate how much effort actually went into his reframing of these portraits, we need to know how much he deliberately erased and what he invented. By returning these images to their historical context, we can begin to appreciate the extent to which Conolly’s essays, as well as the engravings, are historical fictions. With this basis, we can begin to examine what Conolly saw as the specific value of fictional representation in medical discourse.
* * *
The photographs for the thirteen essays came from two sources. The majority were taken by Hugh Welch Diamond (1809-86) at Springfield, the Surrey County Lunatic Asylum.[27] Diamond was a well-known British photographer in the early days of the medium, and he was Alexander Morrison’s successor as Superintendent of the asylum’s female ward from 1848-58, which is why most of his subjects were women. He exhibited his asylum photographs from 1852-59, as “Portraits of Insanity” and similar titles, without commentary on their interpretation. He hoped the normality of the portraits could counteract the popular perception of the insane as wild-eyed maniacs (Burrows and Schumacher 43-44). The patients in his portraits have never been identified, in part because the casebooks for females are missing.[28] The second source is a group of photographs of Bethlem inmates taken by Henry Hering, a print seller whose studio was located near the Hospital.[29] Hering was asked to photograph patients for the private collection of William Charles Hood, the first Medical Superintendent of Bethlem and an acquaintance of both Conolly and Diamond. Hood’s motives for collecting the asylum portraits are unrecorded, but the pictures were not used for exhibition.[30] Most of Hering's photographs were taken at his studio, to which patients were allowed to walk if they were considered well enough. Hood's collection is now in the archive at Bethlem. Most of the photographs are mounted; a diagnosis is written in pencil on the mountings, along with a set of initials for many. Several years ago, Colin Gale, Bethlem archivist, did the basic research of connecting the initials with patient names.[31] Because of his work, we can now identify the subjects of “Religious Mania” and “Religious Melancholia and Convalescence.”
Gilman sees Conolly’s essays on the portraits as of limited value, except that they “supply a series of the missing case studies for some of Diamond’s photographs” (Face 12). From comparing the case notes to the essays, it appears that Conolly was conducting a forensic diagnosis. There is no evidence that he interviewed the patients, or that he even observed them in person at any time. It appears that he worked from the photographs, assisted by some information about the individuals. This may have come from reviewing the case notes, but some of the major details are wrong, suggesting that he may not have read the actual notes and the patient information came secondhand. As the superintendent, Hood would have known the individual cases and may have been Conolly’s source.
“Religious Mania” is an image of Eliza Camplin, born 1820 or 1821 in Lincolnshire, an agricultural district in the English midlands, 150 miles northeast of London.[32] When admitted, she was 36 and living in Stewton, a village in East Lindsey, Lincolnshire, and was married to William Camplin, a laborer. In November or December of 1856, she attended a “Wesleyan Methodist love feast” (a ceremony of food, singing, and testimony popular in the evangelical revival movement of the nineteenth century), and this led to her first attack of “Religious Excitement.”[33] Her condition continued for two months, during which she caused a disturbance in the community; one of her two certificates describes her as “making charges of a serious nature and altogether unfounded against persons of good character.” Her husband authorized her confinement, and she made the trip south to the Hospital in early February 1857. Bethlem required a £100 deposit for each patient, to keep out paupers, which was returned upon discharge, and her security was paid by two neighbors in Stewton, James Bett, a farmer, and P. Oxon, a brick maker. She was admitted on February 9, 1857 in good physical health and placed in the Number One Ward; reserved for the most unmanageable cases, this ward was located on the basement level.[34] The notes describe her as “a woman of inferior education and strong provincial peculiarities.”[35] She suffers from delusions, mainly on religious matters, and “speaks of herself as one peculiarly favoured by the Almighty and denounces almost every other person to hell for not agreeing with [her] ideas.” She is “exceedingly violent, noisy and destructive, very dirty in her habits, very abusive,” and exceptionally foul-mouthed, even for a Bethlem patient. She became worse initially, and grew “noisy at night,” a serious problem at the hospital, where a common gallery communicated with the patient rooms on the ward. Three months later, in May, her mania persisted, but we are told, “her conduct is not so violent, nor is she so spiteful as she was.” According to Conolly’s comments, this would be the date when the first photograph was taken (fig. 4). In September, after seven months’ confinement, she was better at controlling her “violent conduct,” and was moved out of Number One to a “quieter ward.” There, the notes say, she “appears quite sane, but complains much of the treatment she experienced” in the other ward. The second photograph would date from this time, fall of 1857 (fig. 5). The last entry is on October 16, when she remains well, and she was discharged a week later, on October 22, 1857.
Figure 4

Eliza Camplin, photographed by Henry Hering, c. May 1857
Figure 5

Eliza Camplin, photographed by Henry Hering, September or October 1857
Conolly’s two essays on Camplin appeared in the summer of 1858, less than a year after her discharge ("Physiognomy 9"; "Physiognomy 10"). The essays include lengthy meditations on the expressiveness of the human face and the impression it makes on observers, even in the most casual setting:
In each social meeting [. . .] it is in vain to attempt to catch all the momentary shades of expression; but the commonest observation still makes us sensible of their numerous and endless succession. Facial commentaries are unceasingly renewed, not transmitted to words, nor audibly delivered; not intended even to be revealed to the general eye; yet, transient as they are, some visible to all, and all to the adept, and translateable: even producing various degrees of emotional influence on many who are gathered together at the table, or round the evening fire.
"Physiognomy 10" 210b
These transient expressions affect the receiver emotionally, presumably even those that are only visible to the “adept.” Through the recipient’s sensitivity to these impressionistic responses, ephemeral expressions become “translateable,” communicating facts about the emotional and mental state of the person originating them. This same pattern of transmission extends to the photographic reproduction of expressions, whose details “carry the thoughts from the outward signs to the inward and unseen causes” ("Physiognomy 9" 81b). This impressionism defines Conolly’s interpretative method, and he employs it fully in the essays on the images.
His comments on the Camplin photographs are an amalgam of fact, inference, and invention. Camplin’s diagnosis on admission was “Delusions.” It may be that Conolly’s diagnosis of “Religious Mania” seemed more precise, but it also emphasized the central theme of his essays: the social danger of evangelicalism. He added a new ingredient by giving her a marked intelligence, which the case notes do not support. Her residency at Bethlem, he tells us, means that she is more educated and familiar with a greater variety of existence than the generic paupers in the county asylums are. Her face has the “lineaments” of superiority, which she must have inherited from long dead ancestors, giving her signs of a “surpassing intellect” and an “air of superiority” that separates her from “the vulgar” ("Physiognomy 9" 83a). “There is no dullness or rustic stupidity to be seen in her face,” he notes, concluding that she must be “superior to the generality of women of her station” ("Physiognomy 10" 212a). He accounts for this inherited intelligence by relocating her further north, fifty miles closer to Scotland, and describing at length a seemingly unrelated train trip he once made to Edinburgh, during which he observed a gradual change in the physiognomy of the farming population from his train window. Her native intelligence is thus attributed to the northern stock to which she belongs. In fact, her home in the Midlands is less than halfway to Scotland from London.
In Conolly’s version, this superior intelligence was unsatisfied by the quiet life of the hardworking northerners in their “peaceful hamlets,”—self-reliant, God-fearing people who lead honest lives in their picturesque cottages ("Physiognomy 9" 82a). Into this simple, virtuous community comes a dramatic evangelical preacher, seducing the inexperienced locals into “enthusiastic singing, earnest prayers recommended by strenuous physical action, and long sermons, in which the free reins are given to the excited fancy”; such stimuli “attract the common people with a force quite irresistible” ("Physiognomy 9" 82a). The patient exemplifies the consequences faced by a superior intellect in a simple society when suddenly over-stimulated and yielding all self-restraint: her “control of the mind was gone” ("Physiognomy 9" 82b). While this situation may seem distant to his more urbane readership, he corrects this misimpression by attributing her predicament to the vulnerability created by an inferior education. Female education in general is poor, he continues, composed of such “vapid books and songs and occupations” that even modern, so-called educated women are susceptible to religious mania ("Physiognomy 10" 212b). From two photographs and a handful of details, Conolly invents a coherent narrative—technically a morality tale—in which virtue confronts vice and is rescued by the salutary help of the asylum and the diagnostic acumen of its experienced physician.
“Religious Melancholia and Convalescence” followed “Religious Mania” in the sequence, appearing in the next issue. Two images are provided for the subject, a before-and-after sequence, but the historical details for this second patient are sparser than those for the first (fig. 3). He relates that she is 23, her mind overtaxed with theological pondering and the dread produced, once again, by “fanatical preachers” ("Physiognomy 11" 367b). We are not told where she lives or what she does, but we know she suffered “Great mental anxiety, incidental to a responsible charge undertaken by her,” and that this unspecified anxiety caused her attack, the most recent of four ("Physiognomy 11" 368b). No other details are provided. In Conolly’s hands, this patient illustrates the successfulness of moral therapy in a well-run asylum. This trope is present in other essays, as well, but here he ties it directly to the publicity of asylum abuses then current in the newspapers—the essay appeared in print less than two months after the Ruck Commission in Lunacy—complaining that such stories do a serious disservice to modern asylum practices. Of her second image, he explains,
when June came with its genial sunshine, her watchful and kind Physician perceived a return of brightness and activity in his poor patient. Her melancholy thoughts, fixed only on self, disappeared; her mild and amiable character again shone forth; she gratefully acknowledged that her own heart was freed from the pressure of care, and it became her pleasure to console others whose bosoms were still clogged with perilous stuff, and to comfort those still labouring under sadness. Such are among the twice blessed effects of the modern system of treatment of the insane.
"Physiognomy 11" 369a
In this morality narrative, a woman’s misery is remade into happy female selflessness, as the asylum restores her to her essential, Angel-in-the-House nature. Conolly is not talking about an actual person here; he is writing like a novelist, filling in details he could not have known to create a Dickensian narrative of humanitarian benevolence, as if the patient were Oliver Twist recovering in the home of the Maylies.
The woman in "Religious Melancholia" is Eliza Josolyne, born 1832 or 1833. Her two photographs were taken in spring and summer of 1857, about the same time as those of Eliza Camplin. Josolyne was admitted four days after Camplin, on February13, 1857, and was also placed in Number One. It is likely that the two women encountered one another over the next nine months in the common area of the ward. She had three earlier admissions, rather than four. Although her behavior and words are well represented, the case notes do not mention religious melancholia. There is a single reference to religious delusion, in her first admission, five years earlier, but she is diagnosed with mania at that time, not melancholia. The label “Religious Melancholia” is either an error on Conolly's part or an invention, perhaps to tie together the Josolyne and Camplin articles thematically.[36] She came from a large family in Chelsea, Middlesex, headed by John Josolyne, a 50-year-old flour factor.[37] In the 1851 Census, he was married to a much younger woman, Eliza S. Josolyne, age 31, a schoolmistress for young ladies, and they lived with their three daughters, two sons, his mother-in-law and an unrelated child. At age 22, one of the children, Emily, is considerably older than the rest and too old to have a 31-year-old mother. Eliza Josolyne herself was then 18, and the evidence suggests that she and Emily were sisters, while the rest of the children were born to the younger wife.
Eliza Josolyne does not appear in the 1851 Census. She was first admitted to Bethlem that year, at the age of 18, on November 21, 1851, and diagnosed with mania of unknown cause. She is single, a servant with a “moderate education” who can read and write, and her memory is impaired. Little is said of her family in the case register, but her behavior is vividly described:
Very much excited, wild, flighty, and mischievous. Generally quite incoherent. Appears to understand what is said to her but does not give a rational answer and rambles from one thing to another without any reference to the question. Makes a great noise by dancing and jumping about—tears her clothes and throws her things about. Pays no regard to personal cleanliness and is much too unsettled to employ herself with any kind of work. Takes her food very indifferently and is noisy and dirty at nights.[38]
By January, she was getting better and was moved out of the basement to Ward Number Two, on the first floor. In March, she “appears to be quite rational,” and she was discharged as healthy on March 5, 1852.
Four years later, she was readmitted. She had moved from Middlesex to Woolwich, Kent. At the time, her family was living a short distance away, in London. She was 22 and employed as a servant. Starting in April 1856, she became melancholic and at some point attempted suicide. Her parents had her confined on June 16, 1856. One of her securities was provided by J. MacLaren, the headmistress of Sillaclaren School, in Woolwich. MacLaren’s occupation suggests that she may have been a friend or relative of Eliza’s young stepmother and that Eliza was living with her in Woolwich. The medical certificates describe her as despondent—they note a “Constant rolling of the head & body, with a continual low moaning, not speaking or answering any questions.”[39] Her stepmother told the doctors, “she bites her arms and tears her hair” and “attempts to injure herself by beating her head against the wall or floor.” While “Mania” is written across the top of the page, the case notes explain that she is no longer manic, as four years earlier, but is “low and melancholic, sways her body from side to side, covers her face with her hand and utters low moans.” Her face was “sore from pricking it,” and at night, she continued to scratch herself. Her menstrual periods were irregular. Two months later, she was much improved and was discharged on October 31, 1856, after four months of confinement.
Soon after leaving, she obtained a new situation as the only servant in a house that had “some 16 or 20 rooms to keep in order, and the work was of course too hard for her,” as the case notes explain.[40] She became “anxious and then was seized with acute melancholia.” According to her parents, she stopped eating in early February 1857. They confined her hands “to prevent her doing personal violence to herself.” The certifying physician, Thomas Meeres, notes, “She is constantly walking up & down the room piteously moaning.” She was physically healthy but very thin when admitted for the third time, on February 13, 1857, three and a half months after her previous discharge. She slept in the padded room in Number One, because she was knocking her head against doors and walls. Her face was again scratched and “she groans almost without intermission.” This was when Hering took the first of her two photographs, clearly showing the scratches that were omitted from the engraving, as Conolly correctly noted (fig. 6). By March, she was improving and was able to work in the scullery. She recovered slowly throughout the summer, when Hering took the second photograph (fig. 7). By November, the notes state that “she is generally cheerful and always industrious and kind but some days rather dejected.” From January 1858 through August, monthly entries are brief, identical, and uninformative: “no alteration.” At this point, she had been in Bethlem for eighteen months, well beyond the normal one-year limit, so something unusual was taking place. In September, without any known cause, she took a turn for the worse and became “very low” and “desponding.” The essay on her in the Medical Times and Gazette appeared about this time, on October 9, 1858. She became incommunicative and remained that way until Christmas time, when she began to recover and could finally “be induced to answer a question.” By February 1859, fully two years after admission, she was “quite changed and well,” and she continued so in March. Then, on April 29, 1859, there is a one-sentence entry: “She has been recommended for the Incurable List.” This was a special ward at Bethlem that only admitted patients internally. She was transferred there on May 27, 1859, at the age of twenty-five. She remained there until her death fifty years later.[41]
Figure 6

Eliza Josolyne, photographed by Henry Hering, February 1857
Figure 7

Eliza Josolyne, photographed by Henry Hering, summer 1857
Conolly was clearly wrong in many of his basic claims about these two women, but his predictions about them turned out to be accurate, nonetheless. Camplin's condition was, in fact, temporary, as far as we know. According to the 1861 Census, she was back in Stewton living with her husband, along with a two-year-old niece. William Camplin died sometime after 1861, and she eventually moved to Wood Enderby, Lincolnshire, to live with her parents, John and Mary Jeffrey, farmers then in their seventies. The 1871 Census had a column for identifying lunatics, and it was not checked in her case. Her name does not reappear in Bethlem’s admissions lists, suggesting she did not have a reoccurrence. The last trace of her is in the 1881 census, where she is sixty years of age and living alone with her eighty-one-year-old mother in the same village, next door to the rest of the Jeffrey family. In the Josolyne case, Conolly presents her as an example of moral therapeutic success, but he also injects a cautionary note, explaining that many patients in her condition end up returning to the asylum for long-term care, which is exactly what happened.
That these essays were shaped to fit Conolly’s preoccupations may seem cause for censure: he manipulated their cases to promote his own standing in the profession, at the expense of factual accuracy, and he misrepresented the lives and conditions of the individuals in the photographs. The same charges can be leveled against the portraits themselves. Gilman notes that the “photographs give the illusion of reality through the use of existing models” (Face 8). They “possess an aesthetic importance through the skillful manipulation of the format to obtain the greatest effect on the observer.”[42] While framed as documentary evidence, the portraits are carefully lit, with sitters deliberately posing and, at least according to Conolly, selecting their props, like the book held by Camplin (fig. 4). They are an artistic version of reality, and it is possible to understand Conolly’s essays in similar terms, as a written version of the same aesthetic handling of the materials that also promotes the illusion of objectivity.[43]
In essence, by freeing the images from the contingencies of their specific historical context, he redefines them as models for composing his own impressions of aesthetic objects, and so is able to view them as a canvas on which to paint his own impressions. He removes them from the sphere of history to resituate them in the sphere of art. His essays are self-aggrandizing, but they are also self-conscious works of creative writing, fictions masquerading as history in which the power of medical impressionism, and his own acuity as a medical aesthete, plays the central role.
* * *
Conolly’s aesthetic view of images of insanity partially explains his extended engagement with the artistic representation of insanity in A Study of Hamlet. The medical portraits are copies of copies, but even this tenuous link to the real is missing from Hamlet, which belongs unequivocally to the realm of fiction.[44] This distance between pure fiction and life explains why Alfred Hardie freely dismisses Wycherley’s insistence on Hamlet’s madness. The play represents an extreme case for considering the importance of fictionality in psychiatric medicine, and the basic question we need to consider is how a purely imaginary character can compare to a photographic document as a representation of insanity.
Why was Conolly so interested in Hamlet? There were biographical reasons—he spent his early career building a practice in Stratford-upon-Avon, where he seems to have developed a case of Bardolatry (Scull, "John Conolly: Reconsideration" 67). But he was not the only mental physician to write on Hamlet at the time. John Charles Bucknill, Henry Maudsley, and Forbes Winslow, all members of the professional elite, did so as well, and in each case, Hamlet became a case study in the mechanisms of insanity (Bynum and Neve). Conolly's testimony in the Ruck case paralleled his argument in A Study of Hamlet, and so we might consider one of the motivations for his Study as giving himself another chance at public self-justification. He could not defend himself directly against the printed attacks on his character, like Hard Cash, because he feared, and with good reason, provoking more wrongful confinement suits and more damages he could not pay (Scull, "John Conolly: Victorian" 200-1). Thus, he found himself unable to clear his name. In a situation where silence was otherwise prudent, his Study was a safe way to defend both his professional integrity and the soundness of his diagnostic method, and to reach an audience extending beyond the inner circle of professional asylum keepers to a wider community.
Conolly argues that the basic question the play poses is epistemological: how are signs of insanity to be read? The Study focuses on the problem of diagnosis, asking whether Shakespeare “intended simply to portray the feigning of madness, or designedly drew a representation of one of the most delicate of the many shades of a mind really disordered" (Study of Hamlet 1). This is a question of differentiating the fact of insanity from its imitation. Conolly argues that Hamlet's madness is real, the same conclusion reached by other Victorian asylum doctors who wrote on the play, but each physician took a different route to that conclusion.
Conolly's argument hinges on two issues: the definition of insanity and the reliability of bodily signs. Hamlet, he says, is sane at the opening of Act 1, but suffering from the double shock of his father's death and his mother's remarriage. Hamlet is sensitive and unused to such sorrows, and this gives him a "predisposition to actual unsoundness of mind" (22). In such a state, his encounter with the ghost transforms his predisposition into, we are told, "incipient partial insanity" (22). This is Conolly’s primary diagnosis, and he defines it as "a mental condition in which there is a partial disturbance of reason, and that not continual, but fitful, often returning, and productive of perplexing inconsistency of thought and action" (2). When Conolly further qualifies Hamlet's partial insanity as "incipient," then the physical signs of insanity recede even further into the mists of ethereality.
In such liminal cases, a common sign stems from this mixture of rationality and insanity. In incipient cases, sufferers tend to be aware that they are not wholly in control of their actions, and they fear others may notice. "He suspects that he is suspected,” Conolly observes, “and [. . .] declares that [. . .] he has only been pretending to be eccentric, in order to astonish the fools about him [. . .]" (54-55). Hamlet presents this telltale symptom twice—when he warns Horatio and Marcellus that he may "put an antic disposition on," and later, when he tells Rosencrantz and Guildenstern, "I am but mad north-north-west" (2). While the uninitiated literary scholar might see these passages as evidence that Hamlet is "only acting," Conolly assures us that, "The curious mixture of feigned and real madness [. . .] [is] generally only known to those who live much among the insane" (52). Experience teaches the physician that the patient's claim of feigned madness can also be a sign of madness. So too are attempts to offer the asylum doctor proof of sanity by performing sure-fire tests. Patients show how they can do math, or follow instructions, or expound on worldly affairs, and like them Hamlet offers his mother to "bring me to the test / And I the matter will re-word; which madness / Would gambol from" (155). Hamlet's arguments "are precisely such as certain ingenious madmen delight to employ," says Conolly (155). Here and elsewhere, Hamlet's fears of discovery—he suspects that he is suspected—lead him to feign sanity, an "often noticed tendency in lunatics" (86). Acting sane was no proof of sanity in asylum patients, who were frequently devious, using cons that followed predictable patterns, and trying to appear rational was one of the most common. When Conolly testified before the Ruck commission, he took a similar stance, arguing that an important proof of Ruck's delusion was that he covered it up so well.[45]
Ultimately, the externalized signs of insanity are unreliable. Acting mad and saying you are only acting can be a sign of real insanity; acting sane and saying you are sane can also be a sign of insanity. The only sure guide is the experience of the asylum doctor, who can tell a bad copy from the real thing. As Conolly points out, "Persons [. . .] feigning [. . .] madness [. . .] seem generally to have affected merely the look, manner, and actions indicative of silliness or idiocy [. . .]" (66). They never attempt "the more difficult task of copying either the dreadful excesses of real madness, or its marvelous shades of expression, vocal, facial, and muscular, which perhaps defy imitation" (66). These subtleties of madness can never be appreciated by the layperson, and asylum doctors develop a special sensitivity to them only through much experience. There is, in other words, an aesthetic aspect to insanity, and this aspect is its only reliable sign. Conolly is quite clear that what he describes is not simply a subtlety that could be reproduced by skill in dramatic acting. Consider the case of Ophelia. She can be seen in the wards of every asylum, but she is difficult to play well on stage (fig. 8). Missing are "the habitual courtesy [. . .] the glimpses of acute observation," and eight other signs of "things [. . .] imagined by few" (179-80). Without these, "an actress must fail; her gestures, however graceful, will want true expression; her delivery of the words will have the fault of being too pointed and significant; and her singing, however finished and artistic, will want the affecting intonation of a lunatic's song" (180). Insanity manifests in aesthetic qualities, not simple bodily signs, and this is why its symptoms cannot be clearly spelled out in a book. They have to be felt and experienced, rather than logically comprehended. Thus, Conolly focuses on the sensual quality of presentation, not the rational content; he describes the sound, color, and effect of Ophelia—the way her words are delivered and the sensations they produce, rather than what she says. This mode of diagnosis entails opening oneself up to feel the finest shades of affect in response to the asylum patient, so that the asylum doctor is principally defined as a medical aesthete.
Figure 8

Anonymous, photograph by Hugh W. Diamond, c. 1855
An interest in aesthetics appeared in many aspects of Conolly's life, not just in his diagnostic method. His son-in-law, physician Henry Maudsley, noted after Conolly's death that he was "disposed to overestimate those who set forth ordinary reflections in an elegant and easy manner, and to underestimate those who broached profound thought in language sometimes neither easy nor elegant" (173). Similarly, he notes, Conolly's writing style "sometimes affected more the art displayed than the matter contained" (173). In his most well-known remark, Maudsley pointed out Conolly’s defining limitation: "As a writer on insanity, he painted eloquently and pathetically the external feature of the disease, but the philosophical depths of mental phenomena he never cared to sound [. . .]" (172). Maudsley meant to indicate Conolly's shallowness, of course. He was not, as it were, a deep thinker. But in Victorian aestheticism from the Pre-Raphaelites to Oscar Wilde, attention to the sensual qualities of objects is all that matters. Walter Pater repeatedly insisted on the primacy of form, arguing that the object’s meaning lies in its sensual effect on the observer, not in its explicit ideas. To the aesthete, the surface is everything.[46]
The unique interest of Conolly's superficial book on Hamlet lies more in its form than its content. It has a distinctly subjective narrative voice that meditates on problems of reality and fictionality in Hamlet and in the asylum, in art and in life, as he retells the story of Hamlet act by act and scene by scene, describing the development of the Prince’s debility. These meditations tell us about the implied author’s beliefs; they illustrate his skills and even project his personality, so they provide us a clear sense of who is making this argument. This narrator proves to be either a complete fool or incredibly clever. In proving that the Dane’s insanity is real, Conolly describes Hamlet’s unhappy state and concludes, "Such is the canker of the fairest flower of beauty, and of wisdom, and of wit, when the mind becomes diseased; and such are the changes which loving friends shudder to behold [. . .] . And these are not things which a man might play" (120-21). The lyricism and assonance here make the passage unusually compelling; it uses a regular iambic meter that scans like blank verse. So it is easy to forget that the author is talking about a drama, and clearly a man may play such things in art, if not in life. Conolly himself never forgets the theatrical nature of his subject matter; he offers specific stage directions throughout the Study. Implicitly, in arguing that Hamlet represents real rather than feigned insanity, he assumes that real insanity can in fact be feigned: Shakespeare did it successfully in creating Hamlet. And so will the actors who, happily, follow Conolly's well-versed directions.
How are we to reconcile such contradictory claims? Can insanity be feigned or not? Conolly's emphasis on aesthetic forms gives us some help here. In the content of the argument, he says that insanity cannot be feigned. But because he is talking about a play, the essay’s form implies that, in fact, it can. As he notes, Shakespeare successfully imagines the "fine outline" of insanity, a quality we can call the "insanity aesthetic." Because the sign of insanity is ultimately an aesthetic attribute, that is, something more felt than intellectually comprehended, Conolly is saying that works of art, like Hamlet, can succeed in feigning insanity where actions in life must fail.
Conolly's decision to use a play to explain his claims about the signs of insanity is paradoxically right. In a juridical setting, when a physician testifies and a jury has to be convinced, neither he nor any other physician can persuasively argue that the signs of insanity are impossible to spell out and can only be felt. But a claim for an insanity aesthetic can plausibly be made in critiquing a self-defined work of art, and it can also be made in critiquing photographs as aesthetic objects. Ultimately, Conolly is saying exactly the opposite of Alfred Hardie, his avatar’s opponent in Reade's novel. The fact that Hamlet does not exist is the only reason the question of his sanity is truly worth considering.
* * *
Conolly’s actions in the Ruck trial, Rosina Bulwer Lytton’s confinement, and Nottidge v. Ripley all point to a grasping self-centeredness that is hard to forgive, but that same trait is also consistent with his impressionism. By relying on the importance of aesthetic responses, Conolly’s system of medical impressionism necessarily entails comprehending what is objectively seen or heard in self-centered terms, or “to know one’s own impression,” as Pater wrote (viii). Like any form of impressionism, it has its dangers; it runs the risk of confusing interpreter with interpretee, subject with object, even in the most sincere of its practitioners, and Conolly fell into this trap with regularity. Maudsley once remarked of him that, notwithstanding his iconic status as a great and sympathetic humanitarian, "it is certainly true, that the friend of humanity is often imprisoned in a narrow selfism" (156). This is not an unambiguously negative trait; Elaine Showalter observes that, to an unusual degree, Conolly had a "driven identification" with the "insane poor" (47). For asylum doctors, imaginative sympathy was considered necessary to understanding the patient, but it was also recognized as creating an occupational hazard. Bucknill, in his own 1859 study of Hamlet, explains "no one can understand the insane [. . .] who cannot and does not [. . .] throw his mind into them, and sympathize with the state so far as to make it [. . .] during brief periods, almost subjectively his own” (qtd. in Hunter and Macalpine, Three Hundred Years 1067). Asylum doctors, he concludes, lay themselves open to "the seeming contagion of mental disease" (1068).
Clearly, in the asylum essays, Conolly identifies with the represented patients. In A Study of Hamlet, he had many reasons for similarly confusing himself with the object and saying, in essence, Hamlet c'est moi. His Study of Hamlet is a kind of life writing. According to Maudsley, Conolly had "great energy of an impulsive kind [. . .]," but he lacked "the patient tedious labour necessary to carry an event to its best issue," traits that sound very like those of the indecisive Dane (162). Moreover, at this point in his life, he was unable to act in the matter that most concerned him, the problem of his reputation. There is an uncomfortable parallel, too, with Ophelia: all traces but one of Mrs. Conolly simply disappeared from the historical record soon after 1839 when they moved to the Hanwell Lunatic Asylum.[47] The exception is dated 1866, when a death certificate identified her as a roomer in a London neighborhood for transients. For Conolly, I would suggest, the play Hamlet was real because he saw in it his own reflection, and so it became as real to him as the ghost of Hamlet’s father, an apparition in the play that goes completely unremarked in Conolly's discussion of Hamlet's delusions.
But what of Charles Reade? Ultimately, both The Physiognomy of Insanity and A Study of Hamlet are more calculated treatments of the problematic relationship between representation and the real than the comment from Hard Cash with which we began. Still, it would be a mistake to reduce Reade's novel to the line, "A man must exist before he can be insane." The character who makes this statement is himself a fictional character, and his entire argument—about the inability of art to represent the real—is incorporated into Reade's unique art form, the "matter-of-fact Romance" that folded documentary evidence, like the newspaper reports of Conolly's trial, into fictional stories. The statement tells against itself, reinforcing the view that in fact the real can be represented in fiction. Neither one of these two writers takes a straightforward view of fictionality, but one conclusion we can draw from this is that Hard Cash was in fact engaged with the same questions about art and its role in the representation of the real as the Study of Hamlet it satirized.
As a novelist, Reade’s decision to take up the question of art’s relationship to the real left him safely within the boundaries of the Victorian novelist’s accepted role, since fiction writers asserted the artistic right to represent “real life” in their writing. However, for a physician to consider the same question of art’s ability to represent life was clearly stepping beyond the perimeter of professional expertise. The novelist might critique the function of art, but the physician’s knowledge was tied to the concrete realm of human physicality.
In this regard, Conolly’s treatment of both Shakespeare’s play and photographic portraiture were Victorian equivalents of interdisciplinarity. He is clearly aware of his position as an interloper, and he makes a sustained effort to circumscribe his engagement with the sphere of art and artistry to questions of mental medicine, rather than those of artistic value. For this reason, the centrality of aesthetic impressionism to his writing can seem surprising by contemporary standards, as can its evident lack of controversy to the professionals who made up most of Conolly’s readership. The appeal to impression is commonplace in mid-Victorian psychiatric writing. While sometimes represented as a newly acquired intuitive sense or the wisdom of accumulated experience, in Conolly’s hands it becomes an acute perceptiveness, honed through years of practice. This sensitivity enables him to see, hear, and feel the signs of madness more clearly than the uninitiated. Such exceptional sensitivity positions him as one of those special beings, “different in degree but not in kind,” described by William Wordsworth. But Conolly is not claiming to be a poet or artistic producer. He is more like the critic, a sensitive consumer of sensations, and so his role has a closer parallel to the subjective mode of assessment at the heart of Pater’s aesthetic criticism than the expressionism of Wordsworth.
To call Conolly an “aesthete” is ultimately not a claim for his own interdisciplinarity so much as an acknowledgment of our present-day disciplinary limitations. Few historians of medicine are taught the philosophy of aestheticism. Victorian literature students are systematically trained in neither historiography nor the history of medicine. Of those that do study the field, few have practiced extended critical engagement with medical texts, more often relying on secondary literature for summary and context.[48] Given the current disciplinary geographies of history and literature, the prominence of aestheticism in the practice of Victorian mental medicine goes unremarked, largely because those who read the primary texts are unfamiliar with the concept and those who know the concept do not read the medical texts. The result is a diminished view of literature and art in medical history, and a correlative perception in literary study of aestheticism as unrealistically detached from the social conditions of its historical practice.
To suggest that interdisciplinarity can or will solve this and other intellectual aporias generated by disciplinary distinctions is overly idealistic. McWilliam suggests that “too much might be expected of interdisciplinarity,” if we see it as a panacea for our intellectual divisions (21). Scholars on the development of the professions in nineteenth-century Britain have been remarkably compelling in demonstrating the importance of disciplines and their monopolistic claims to expertise on specific bodies of knowledge, and the pattern remains valid.[49] Thus, imagining that individual disciplines can or will give up their proprietary methodologies verges on an ahistoricity that, itself, contradicts the attempts of interdisciplinary literary scholars to become better historians.
The challenge presented by Conolly’s writing on art is thus borne of our own professional divisions; however necessary and enabling, they also consign “hybrid” works, like medical writing on art, to the limbo of disciplinary monstrosity. There is, I would argue, a promise of new knowledge in research that targets neither-fish-nor-fowl documents. Because they challenge present categories of knowledge rather than past ones, these documents suggest the extent to which our current understanding of Victorian culture contains the fetish of the present. At the same time, they expose new possibilities for considering how our most disparate categories, like medicine and aesthetics, enjoyed a more intimate contact historically than we could ever imagine.
Appendices
Biographical notice
A specialist in nineteenth-century British literature, Logan teaches at Temple University. His study of ideas about cultural evolution and the mind, Victorian Fetishism: Intellectuals and Primitives, is due out from SUNY Press in late 2008. He is also General Editor of the Blackwell Encyclopedia of the Novel, scheduled for publication in 2010.
Notes
-
[1]
See Suzuki 87. McCandless identifies 1858-59 as the height of the second lunacy panic, but given the prominence of the 1862 Windham case in the London papers, the issue had clearly not faded away. Wilkie Collins’s The Woman in White also features an unjust confinement in a lunatic asylum; Reade’s novel immediately followed it as the syndicated novel in Charles Dickens’s All the Year Round.
-
[2]
On Charles Reade’s writing, see Poovey; Sutherland; Elwin; Burns; Phillips.
-
[3]
Throughout this essay, I use the term insanity to reference statements about madness within Victorian medical discourse, not insanity as such.
-
[4]
See Gilman, Disease and Representation 18-30.
-
[5]
Robert Gardiner Hill, head of Lincoln Asylum, was the first physician to claim to have abolished restraint entirely, and he discussed his methods in his Lecture on the Management of Lunatic Asylums and the Treatment of the Insane (1839). Conolly visited Gardiner Hill at Lincoln as he was preparing to take up his duties at Hanwell in 1839.
-
[6]
There are no full-length biographies of Conolly. For information on his life and career, see: Scull et al., Masters of Bedlam; Scull, "John Conolly”; Maudsley.
-
[7]
She recounts the abduction in her memoir, A Blighted Life. The incident is discussed in Sutherland, Victorian Fiction. See also Small, Love's Madness 144-50.
-
[8]
Lytton, Blighted Life 43. On Conolly's role in the Lytton case and his relationship with Charles Dickens, publisher of Hard Cash, see Sutherland, Victorian Fiction ch. 3.
-
[9]
Showalter discusses this change in Conolly’s reputation (47-48). She suggests that his son-in-law, Henry Maudsley, promoted the view of him as hypocritical, but more recent work has tended to reinforce the idea that Conolly’s principles changed with his financial situation. See Scull, “John Conolly.”
-
[10]
The civil trial took place on June 21-23, 1859. The Commission in Lunacy was held the previous year, on Aug. 23-27, 1858. For full accounts of the Commission, see “Commission in Lunacy,” Journal of Mental Science; the daily accounts in the Times (“Commission in Lunacy”) are more detailed. On the trial, see the two accounts in the Journal of Psychological Medicine (“Ruck v. Stilwell” and “Unlawful Detention”) and the daily reports in the Times (“Ruck v. Stilwell”). For critical commentary, see Suzuki, Madness at Home 144-50. See also Hunter and Macalpine, "Dickens and Conolly." Many of the sources for Reade’s Wycherley quotations, including minor details like his references to Pascal and John Howard, are drawn from Conolly’s Inquiry Concerning the Indications of Insanity (1830). Others come from Conolly’s Treatment of the Insane without Mechanical Restraints (1856).
-
[11]
"Commission in Lunacy," Times 25 Aug. 1858: 5f.
-
[12]
Ibid.: 6a; "Unlawful Detention," 626-27.
-
[13]
9 George 4, c.41.
-
[14]
"Ruck v. Stilwell," Times 24 June 1859: 11d.
-
[15]
During Conolly’s generation, psychiatrists were still struggling with ways to earn money beyond the modest livings usually afforded by asylum keeping. The next generation discovered the much more profitable practice of charging consultation fees for meetings with wealthy but troubled individuals who were not institutionalized.
-
[16]
This clarification was written into the Lunacy Acts Amendment Act of 1862 (25 & 26 Vict., c. 111 s. 24).
-
[17]
I am indebted to Carson’s unpublished paper for information in this paragraph on the problems in definitions of insanity (9).
-
[18]
Conolly’s early ideas about insanity are spelled out in An Inquiry Concerning the Indications of Insanity. For an analysis of the key parts of the Inquiry and the professional forces that motivated it, see Suzuki ch. 3. See also Scull, "Victorian Alienist.”
-
[19]
Scull, "Victorian Alienist." On the Nottidge case, see Schwieso.
-
[20]
In On Obscure Diseases of the Brain (1860). Qtd. in Hunter and Macalpine, Three Hundred Years 1075.
-
[21]
“Commission in Lunacy,” Times 28 Aug. 1858: 11b.
-
[22]
Ibid.
-
[23]
The photographs and some engravings are reproduced in two sources: Burrows and Schumacher; Gilman, Face.
-
[24]
Conolly, "Physiognomy 1” 3a.
-
[25]
See Burrows and Schumacher. And see Gilman, Face.
-
[26]
The Bethlem Royal Hospital Archives and Museum houses all of the casebooks for the hospital. In the 1850s and 1860s, monthly entries were the rule, except in times of crisis. This was far better than the casebooks of Surrey County Asylum (Springfield), which used annual entries. Most of their Victorian records are archived at the Surrey History Center, Woking.
-
[27]
For details of Diamond’s life and career, see Bloore, Burrows and Schumacher 6-21, and Gilman, Faces 3-11.
-
[28]
The casebooks for males are archived at the Surrey History Center.
-
[29]
Burrows and Schumacher identify it as 137 Regent Street (51n7).
-
[30]
Gale and Howard 12. Hering sold one of the photographs in 1863 to Charles Darwin, who used it in his Expression of the Emotions in Man and Animals.
-
[31]
While Gale has no further plans to publish his finding, he has made them available in the catalogue of the Bethlem Royal Hospital Archives and Museum, at http://www.bethlemheritage.org.uk/web/HPA.htm.
-
[32]
Census Returns of England and Wales, Kew, Surrey, England, 1861.
-
[33]
Female Patient Casebook, 1857, CB-071, Box A03/4, Patient Casebooks, Bethlem Royal Hospital Archives and Museum.
-
[34]
The most comprehensive source for information on Bethlem is by Andrews. See also Gale and Howard 3-15.
-
[35]
Female Patient Casebook, 1857, CB-071, Box A03/4, Patient Casebooks, Bethlem Royal Hospital Archives and Museum.
-
[36]
The diagnosis in the casebook and on the original photograph is “acute melancholia.” While familiar with the Hering collection at Bethlem, Burrows and Schumacher have silently retained Conolly’s erroneous label.
-
[37]
The 1851 Census lists his occupation as “Commission Agent.” The additional detail of being a flour merchant comes from the Bethlem case register.
-
[38]
Female Patient Casebook, 1851, CB-055, Box A04/7, Patient Casebooks, Bethlem Royal Hospital Archives and Museum.
-
[39]
Female Patient Casebook, 1856, CB-069, Box A03/4, Patient Casebooks, Bethlem Royal Hospital Archives and Museum.
-
[40]
Female Patient Casebook, 1856, CB-071, Box A03/4, Patient Casebooks, Bethlem Royal Hospital Archives and Museum.
-
[41]
Personal conversation with Colin S. Gale, Senior Archivist at Bethlem Royal Hospital Archives and Museum, Sept. 2006. Gale located this information in the casebooks for Bethlem’s ward for incurables.
-
[42]
Gilman, Face 9. Gilman refers to Diamond’s photographs, but since he misattributes the Hering prints to Diamond, the remark clearly extends to them as well.
-
[43]
Orvell gives an important analysis of this pattern in photography.
-
[44]
Shakespeare based Hamlet on a story in Belleforest’s Histoires Tragiques (1576), which was itself based on a story originating in Norse mythology that appeared in the Historia Danica of Saxo Grammaticus (c. 1200; printed 1514).
-
[45]
“Commision in Lunacy,” Times 27 Aug. 1858: 7b.
-
[46]
The central text on surfaces in Victorian aestheticism is Walter Pater’s Studies in the History of the Renaissance, first published 1873. His clearest statement on the imperative value of form appears in his discussion of the School of the Giorgionne. Parts of Renaissance were printed earlier, beginning with his 1867 essay on Wincklemann in Westminster Review.
-
[47]
On the fate of Mrs. Conolly, see E. Burrows.
-
[48]
I discuss this problem and document it in "Literature and Medicine: Twenty-Five Years Later."
-
[49]
On the medical profession, see Waddington.
Works Cited
- Andrews, Jonathan, ed. The History of Bethlem. New York: Routledge, 1997.
- Bloore, Carolyn. Hugh Welch Diamond, 1808-1886: Doctor, Antiquarian, Photographer. Richmond: London Borough of Richmond upon Thames, 1980.
- Burns, Wayne. Charles Reade: A Study in Victorian Authorship. New York: Bookman, 1961.
- Burrows, Adrienne, and Iwan Schumacher. Portraits of the Insane: The Case of Dr. Diamond. London: Quartet Books, 1990.
- Burrows, Elizabeth. "Alienists' Wives: The Unusual Case of Mrs. John Conolly." History of Psychiatry 9.35 (1998): 291-301.
- Bynum, W. F., and Michael Neve. "Hamlet on the Couch." Bynum, Porter, and Shepherd 289-304.
- Bynum, W. F., Roy Porter, and Michael Shepherd, eds. The Anatomy of Madness: Essays in the History of Psychiatry. Vol. 1. London: Tavistock, 1985.
- Carson, John. "Theaters of Proof: Mind and Its Experts in the Nineteenth-Century English Courtroom." Unpublished essay, 2006.
- Census Returns of England and Wales. Kew, Surrey, England.
- "Commission of Lunacy on Mr. Ruck." Journal of Mental Science 5.27 (1858): 122-46.
- "Commission in Lunacy on Mr. Ruck." Times, 24 Aug. 1858: 10b-d; 25 Aug.: 5e-6a; 26 Aug.: 7a-c; 27 Aug.: 8e-9a; 28 Aug.: 11a-b.
- Conolly, John. An Inquiry Concerning the Indications of Insanity, with Suggestions for the Better Protection and Care of the Insane. London: J. Taylor, 1830.
- Conolly, John. "The Physiognomy of Insanity: No. 1, Religious Melancholy." Medical Times and Gazette NS 16 (1858): 2-4.
- Conolly, John. "The Physiognomy of Insanity: No. 9, Religious Mania." Medical Times and Gazette NS 17 (1858): 81-83.
- Conolly, John. "The Physiognomy of Insanity: No. 10, Religious Mania—Convalescence." Medical Times and Gazette NS 17 (1858): 210-12.
- Conolly, John. "The Physiognomy of Insanity: No. 11, Religious Melancholia." Medical Times and Gazette NS 17 (1858): 367-69.
- Conolly, John. A Study of Hamlet. 1863. New York: AMS, 1973.
- Elwin, Malcolm. Charles Reade. New York: Russell, 1969.
- Esquirol, Jean Etienne Dominique. Des maladies mentales, considérées sous les rapports médical, hygienique, et médico-legal. Paris: Ballière, 1838.
- Gale, Colin, and Robert Howard. Presumed Curable: An Illustrated Casebook of Victorian Psychiatric Patients in Bethlem Hospital. Petersfield, UK: Wrightson Biomedical Publishing, 2003.
- Gilman, Sander L. Disease and Representation: Images of Illness from Madness to Aids. Ithaca: Cornell UP, 1988.
- Gilman, Sander L., ed. The Face of Madness: Hugh W. Diamond and the Origin of Psychiatric Photography. New York: Brunner/Mazel, 1976.
- Haslam, John. Medical Jurisprudence: As It Relates to Insanity, According to the Law of England. In Tracts on Medical Jurisprudence. Ed. Thomas Cooper. Philadelphia: J. Webster, 1819. 281-348.
- Hill, Robert Gardiner. A Lecture on the Management of Lunatic Asylums and the Treatment of the Insane. London: Simpkin, Marshall, 1839.
- Hunter, Richard, and Ida Macalpine. "Dickens and Conolly: An Embarrassed Editor's Disclaimer." Times Literary Supplement Aug. 11, 1961: 534-35.
- Hunter, Richard, and Ida Macalpine. Three Hundred Years of Psychiatry, 1535–1860: A History Presented in Selected English Texts. London: Oxford UP, 1963.
- Logan, Peter Melville. "Literature and Medicine: Twenty-Five Years Later." Literature Compass (forthcoming 2008).
- Lytton, Rosina Bulwer. A Blighted Life: A True Story. Bristol, England: Thoemmes P, 1994.
- Maudsley, Henry. "Memoir of the Late John Conolly, M.D." Journal of Mental Science 12.58 (1866): 151-74.
- McCandless, Peter. "Liberty and Lunacy: The Victorians and Wrongful Confinement." Madhouses, Mad-Doctors and Madmen: The Social History of Psychiatry in the Victorian Era. London: Athlone, 1981. 339-62.
- McWilliam, Rohan. "What Is Interdisciplinary About Victorian History Today?" 19: Interdisciplinary Studies in the Long Nineteenth Century 1 (2005). 19 Feb. 2008 http://www.19.bbk.ac.uk.
- Morrison, Alexander. Outlines of Lectures on Mental Diseases. 2nd ed. London: Longman, 1826.
- Orvell, Miles. The Real Thing: Imitation and Authenticity in American Culture, 1880-1940. Cultural Studies of the United States. Chapel Hill: U of North Carolina P, 1989.
- Pater, Walter H. Studies in the History of the Renaissance. London: Macmillan, 1873.
- Phillips, Walter C. Dickens, Reade, and Collins: Sensation Novelists. New York: Columbia UP, 1919.
- Poovey, Mary. "Forgotten Writers, Neglected Histories: Charles Reade and the Nineteenth-Century Transformation of the British Literary Field." ELH 71 (2004): 433-53.
- Reade, Charles. Hard Cash: A Matter-of-Fact Romance. London: Chatto and Windus, 1927.
- "Ruck v. Stilwell and Another." Journal of Psychological Medicine and Mental Pathology 12.2 (1859): 571-74.
- "Ruck v. Stilwell." Times, 22 June 1859: 11b-c; 23 June: 9c-e; 24 June: 11b-d.
- Schwieso, Joshua John. "'Religious Fanaticism' and Wrongful Confinement in Victorian England: The Affair of Louisa Nottidge." Social History of Medicine 9.2 (1996): 159-74.
- Scull, Andrew. "John Conolly: A Reconsideration." Journal of the Royal Society of Medicine 81 (1988): 67-71.
- Scull, Andrew. "John Conolly: A Victorian Psychiatric Career." Social Order/Mental Disorder: Anglo-American Psychiatry in Historical Perspective. Berkeley: U of California P, 1989. 164-212.
- Scull, Andrew. The Most Solitary of Afflictions: Madness and Society in Britain, 1700-1900. New Haven: Yale UP, 1993.
- Scull, Andrew. "A Victorian Alienist: John Conolly, Frcp, Dcl (1794-1866)." Bynum, Porter, and Shepherd 103-50.
- Scull, Andrew, Charlotte MacKenzie, and Nicholas Hervey, eds. Masters of Bedlam: The Transformation of the Mad-Doctoring Trade. Princeton: Princeton UP, 1996.
- Showalter, Elaine. The Female Malady: Women, Madness, and English Culture, 1830-1980. New York: Penguin, 1985.
- Small, Helen. Love's Madness: Medicine, the Novel, and Female Insanity, 1800-1865. Oxford: Clarendon, 1996.
- Sutherland, John. Victorian Fiction: Writers, Publishers, Readers. New York: St. Martin's P, 1995.
- Suzuki, Akihito. Madness at Home: The Psychiatrist, the Patient, and the Family in England, 1820-1860. Berkeley: U of California P, 2006.
- Taylor, Jenny Bourne, and Sally Shuttleworth, eds. Embodied Selves: An Anthology of Psychological Texts: 1830-1890. Oxford: Clarendon, 1998.
- "Unlawful Detention in a Lunatic Asylum, Ruck V. Stillwell and Another." Journal of Psychological Medicine and Mental Pathology 12.2 (1859): 615-34.
- Waddington, Ivan. The Medical Profession in the Industrial Revolution. Dublin, Ire.: Gill, 1984.
List of figures
Figure 1
Plate 8, “Religious Mania”
Figure 2
Plate 9, “Religious Mania: Convalescence”
Figure 3
Plate 10, “Religious Melancholia and Convalescence”
Figure 4
Eliza Camplin, photographed by Henry Hering, c. May 1857
Figure 5
Eliza Camplin, photographed by Henry Hering, September or October 1857
Figure 6
Eliza Josolyne, photographed by Henry Hering, February 1857
Figure 7
Eliza Josolyne, photographed by Henry Hering, summer 1857
Figure 8
Anonymous, photograph by Hugh W. Diamond, c. 1855