
Résumés
Abstract
The study aimed to determine whether the incidence and duration of certified sick leave (CSL) among nurses had increased during major restructuring of the health care system in the province of Québec, and to determine whether nurses exposed to adverse psychosocial factors at work showed an increased incidence of CSL. It involved nurses working in 13 health facilities. Sickness absence data were retrieved from administrative files (n = 1454). Incidence of CSL for all diagnoses and for mental health problems was examined. Telephone interviews were conducted to measure psychosocial factors at work with validated instruments. There was an increase in CSL among nurses during the restructuring, particularly for mental health problems. Modifiable adverse psychosocial work factors were identified and provide basis for interventions. Since human resources are the mainstay and primary resource of the health network, it is essential that people be able to perform their work under optimal conditions.
Résumé
La plupart des pays industrialisés connaissent une augmentation importante des absences du travail pour des problèmes de santé mentale. Le tiers de ces absences serait relié au travail et aux conditions dans lesquelles il s’exerce. De plus, les effets du travail sur la santé des personnes, notamment la santé mentale, seraient grandement sous-estimés et si un renversement des tendances (dans les conditions d’exécution du travail) ne survient pas, dans un délai raisonnable, les coûts économiques et sociaux de ce dérapage deviendront insupportables, tant pour les travailleurs que pour les entreprises et pour les caisses d’assurance privées ou publiques.
Certains facteurs psychosociaux au travail sont reconnus pour leur contribution potentielle à la survenue des problèmes de santé mentale chez les travailleurs et travailleuses. Les deux modèles les mieux documentés dans ce domaine sont ceux de la demande psychologique, la latitude décisionnelle et le soutien social de Karasek, Theorell et Jonhson et celui du déséquilibre entre les efforts et la reconnaissance de Siegrist. Une combinaison de ces modèles théoriques permet de faire un diagnostic des facteurs particulièrement nocifs pour la santé et offre aux gestionnaires un cadre de référence stimulant susceptible de soutenir l’action.
Le contexte. La dernière décennie a connu d’importantes réformes dans le réseau québécois de la santé dans un souci d’améliorer l’efficacité du système et d’en réduire les coûts. De façon générale, l’environnement psychosocial du travail s’est détérioré pendant la transformation du réseau.
Les objectifs. Un premier objectif de cette étude visait à déterminer si l’incidence et la durée des absences pour maladie certifiées (AMS) chez les infirmières avaient augmenté pendant la transformation du réseau de la santé. À cette fin, les absences pour maladie tous diagnostics et pour un problème de santé mentale ont été examinées selon les différentes périodes caractérisant la transformation. Un deuxième objectif visait à déterminer si les infirmières exposées à des contraintes psychosociales au travail (mesurées par entrevue) pendant la transformation, avaient une augmentation d’AMS sur une période de 17 mois.
Les méthodes. Cette étude comporte six ans de suivi (1993–1999) des absences pour maladie certifiées (recueillies dans les dossiers administratifs) chez les infirmières de 13 établissements de santé de la région de Québec. La population à l’étude comprenait les infirmières avec un statut permanent d’emploi en avril 1995, lorsque la restructuration a commencé. Parmi elles, 2 878 étaient encore active à l’automne 1997, lorsque l’étude a débuté et 374 avaient pris leur retraite entre 1995 et 1997. L’étude comportait également un suivi de 17 mois des AMC chez les infirmières actives qui ont été invitées à participer à une entrevue téléphonique sur la santé et les facteurs psychosociaux au travail.
Les résultats. Au cours du suivi, 52 % des infirmières se sont absentées au moins une fois pour maladie avec un certificat médical. Parmi ces absences, les deux tiers se rapportaient à des diagnostics « potentiellement reliés à l’environnement psychosocial du travail ». Parmi ces diagnostics, les problèmes de santé mentale étaient les plus fréquents (25 %) et ceux qui duraient le plus longtemps (70 jours en moyenne).
Il y a eu une augmentation non significative de l’incidence des absences pour maladie certifiées (AMC) et une augmentation significative de leur durée jusqu’à la deuxième année après la restructuration alors que les absences duraient en moyenne 24 jours de plus qu’avant la restructuration. Pour les problèmes de santé mentale, il y a eu une augmentation significative de l’incidence et de la durée des AMC. La moyenne de la durée de ces absences a augmenté jusqu’à l’année après la restructuration puis a diminué mais est restée supérieure de 24 jours à la moyenne de base, avant la restructuration.
Les facteurs psychosociaux associés à une augmentation de l’incidence d’AMC tous diagnostics étaient : un faible niveau de latitude décisionnelle, de soutien social, de reconnaissance, toutes les combinaisons de tension au travail et un déséquilibre effort/reconnaissance. Les infirmières dans un emploi qui combinait une demande faible, à un manque de latitude et de reconnaissance avaient le plus haut risque d’AMC. Les infirmières qui rapportaient un niveau élevé de reconnaissance n’étaient plus à risque de s’absenter et ce, quel que soit le niveau de tension au travail rapporté. Les absences pour un problème de santé mentale étaient associées à une demande élevée, un manque de soutien social et de reconnaissance, une combinaison de demande élevée avec une latitude faible ou élevée, et un déséquilibre effort/reconnaissance.
Conclusion. La présente étude montre qu’il y a eu une augmentation significative de la survenue et de la durée des absences pour maladie certifiées chez les infirmières pendant la transformation du réseau. Ceci est particulièrement vrai pour les absences pour un problème de santé mentale. Ces résultats supportent l’idée que d’importants changements dans l’environnement de travail devraient être planifiés attentivement afin de prévenir la détérioration des facteurs psychosociaux dont l’impact sur la santé et leurs absences ont été documentés.
Pour favoriser des milieux de travail sains et productifs, il est important, entre autres voies, d’intégrer des préoccupations et des objectifs de santé dès la conception d’un changement organisationnel et de poursuivre des objets d’intervention préventive. Le meilleur moyen d’assurer la santé mentale des travailleurs et des travailleuses est d’agir sur les facteurs qui contribuent davantage au développement d’un milieu de travail sain et respectueux des personnes et sur lesquels les organisations sont en mesure d’intervenir efficacement. Or, les facteurs organisationnels qui offrent les meilleures garanties de santé mentale sont : une organisation du travail qui sait doser correctement la charge de travail et l’autonomie décisionnelle; des conditions de travail qui permettent de mieux composer avec les exigences de la vie moderne; des gestionnaires qui privilégient la transparence des communications, qui sont à l’écoute des employés et qui savent détecter les conflits naissants et les gérer; une culture organisationnelle qui valorise le respect des personnes, reconnaît leur contribution, évite la compétition excessive et investit à long terme dans son capital humain.
Resumen
Este estudio trata de determinar si la incidencia y la duración de las ausencias por enfermedad certificada (AEC) de las enfermeras se han incrementado durante la gran reestructuración del sistema de salud en la Provincia de Quebec, y determinar si las enfermeras expuestas a factores sicosociales adversos en su trabajo muestran una incidencia incrementada de AEC. Participan enfermeras de 13 establecimientos de salud. Los datos de enfermedad fueron tomados de los archivos administrativos (n = 1454). Se examinó la incidencia de AEC por todos los diagnósticos y por los problemas de salud mental. Se efectuaron entrevistas telefónicas para medir los factores sicosociales en el trabajo mediante instrumentos validos. Hubo un incremento en la AEC de las enfermeras durante la reestructuración, particularmente por causa de problemas de salud mental. Se identifico factores sicosociales adversos de trabajo, potencialmente modificables, y se procuro las bases para futuras intervenciones. Puesto que los recursos humanos son el pilar y recurso principal del sistema de salud, es esencial que el personal sea capaz de desarrollar su trabajo en condiciones optimas.
Corps de l’article
Since the early nineties, most industrialized countries have seen an increase in sick leave from work due to mental health problems (Karttunen, 1995; Schaufeli and Kompier, 2001; Vézina, 1998). One-third of these absences are potentially related to work and working conditions (Vézina et al., 1992). In a recent book on Work, Organization and Health, Vinet shows that the effects of work on health, and on mental health specifically, are greatly underestimated and if there is no trend reversal (in the conditions of work execution) in a reasonable time limit, the economic and social costs of this blunder will become intolerable as much to the workers, as to the organizations and private or public health disability insurance providers (Vinet, 2004: 314).
Certain psychosocial factors at work are now recognized as potential contributors to the incidence of mental health problems among workers (Sauter, Murphy and Hurrell, 1990; Vézina et al., 1992). The two most frequently documented models on adverse psychosocial work factors are Karasek and Theorell’s demand-control model (Karasek and Theorell, 1990) and the effort-reward imbalance model defined by Siegrist (Siegrist, 1996). The first postulates an association between health problems and job strain at work incurred by a combination of high psychological demands and low decision latitude. It further hypothesizes that social support at work reduces the health effect of job strain on health (Johnson, Hall and Theorell, 1989). The second model stipulates that a work situation characterized by a combination of high extrinsic efforts and low rewards (ERI) is accompanied by emotional and physiological pathological reactions (Siegrist, 1996). Furthermore, intrinsic effort is hypothesized to modify the association between ERI and health problems (Siegrist, 1996). A combination of these theoretical models renders possible a diagnosis of a combination of factors particularly harmful to health, and offers managers stimulating terms of reference to sustain action “to act differently” rather than withdrawal or abdication (Vinet, 2004: 339–40).
Background
Restructuring and Downsizing
The past decade has been one of sweeping reform within Québec’s provincial health-care system, as part of an effort to cut health-care costs and improve efficiency. In general, psychosocial factors at work deteriorated during the network transformation (Bourbonnais et al., 2005). Nurses have reported a considerable increase in the prevalence of psychological demands (from 53% in 1994 to 66% in 1998) and combined high demands/low latitude (from 30% to 35%), as compared with a sample of nurses studied in 1994. They also reported a higher prevalence of psychological demands, low decision latitude, psychological distress, use of prescribed psychotropic medication and health average or poor compared to people of the same age, than did a representative sample of the general female working population of the province of Quebec in 1998 (Bourbonnais et al., 2005).
Intensified psychosocial constraints at work were also reported by researchers in studies of similar hospital restructuring contexts, both in Canada (Greenglass, Burke and Fiksenbaum, 2001, 2002; Woodward et al., 2000) and elsewhere (Matteson and Ivancevich, 1990). Workstation changes were identified as stressful because they involve ruptured social relationships and transformations in work routine and demands (Gerpott, 1990).
Although psychosocial factors have been extensively studied in conjunction with absenteeism in stress, management, industrial and organizational psychology literature (van der Doef and Maes, 1999; Xie and Schaubroeck, 2001), most such studies have addressed absenteeism for any cause or reason and for any duration, including short absences that may not be specifically related to health (Harrison and Martocchio, 1998; Johns, 1997). Yet, medically certified sick leave is recognized as a more valid indicator of sickness (Bourbonnais and Vinet, 1989; Kivimäki et al., 2003; Marmot et al., 1995). According to Marmot et al. (1995), medically certified sick leave serves as a measure of health among the working population when health is understood to be a mixture of social, psychological and physiological functioning. Kivimäki et al. (2003) reported evidence linking sick leave to mortality, thereby indicating that routinely-documented, medically-certified absences could be used as a global measure of health differentials among employees.
Moreover, studies of the psychosocial work environment have primarily focused on sick leave for all diagnoses (Niedhammer et al., 1998; North et al., 1996) and few have specifically examined certified sick leave due to mental health problems (Bosma et al., 1997; Bourbonnais and Mondor, 2001; Stansfeld, Fuhrer et al., 1997; Stansfeld, Rael et al., 1997). Only one study has examined the effect of change in psychosocial work factors on medically certified sick leave from work. A seven-year follow-up of municipal employees subjected to downsizing revealed that the highest risk of sick leave for all causes was associated with the combined effects of poor latitude or negative changes in job control, demands and social support (Kivimäki et al., 2000; Vahtera et al., 2000). No previous study has documented the evolution of the incidence and duration of certified sick leave specifically for mental health problems during major restructuring.
A first objective of this study was to determine whether the incidence and duration of certified sick leave (CSL) among nurses had increased during the health care restructuring. To that end, the incidence and duration of CSL for all diagnoses and that for mental health diagnoses were examined over a 6-year period broken down into sub-periods that characterize the restructuring timeframe. A second objective was to determine whether nurses exposed to adverse psychosocial factors at work (measured by interview) during restructuring, showed an increased incidence of certified sick leave over a 17-month period.
The Study
Study Design and Population
This longitudinal study involved a six-year follow-up of certified sick leave among nurses working in 13 health facilities in the Québec City area (six acute-care hospitals, two long-term care hospitals and five local community health care centres). No control group was available since the restructuring affected the health sector province-wide. A list of all eligible nurses was provided by the human resources department in each institution. The Commission for Access to Information ruled in favour of the researcher’s request for personal information concerning study participants. The study population (recruited on a voluntary basis) was comprised of unionized nurses with permanent status as of April 1995 (n = 3,152), at baseline, when the restructuring began. Among them, 2878 were still active in fall 1997, when the study began, and 374 had retired between 1995 and 1997. The study also involved a 17-month follow-up of certified sick leave among active subjects in September 1997 who were invited to participate in a telephone interview on health and psychosocial work factors.
Data Collection
Certified sick leave. For each nurse who provided written consent, data for all occurrences of certified sick leave (CSL) (first and last day of each spell) during the 6-year period, was collected by a research assistant from each health care facility’s administrative records. The CSL policy was verified for uniformity across the facilities. No changes were made to the policy during the study period. The systematic recording of sick leave in each hospital taking part in the study was also verified, and insured the reliability and completeness of the data. CSL were defined as absences lasting more than three days requiring a medical certificate issued by a general practitioner unconnected with the organization or the research. The diagnoses were coded in two categories according to a procedure validated in previous studies (Bourbonnais and Vézina, 1995; Bourbonnais et al., 1992): (1) mental health and somatic problems — “potentially related to psychosocial work factors” — such as burnout, anxiety, depression, emotional disorders, excessive fatigue, severe sleeping disorders, musculoskeletal or cardiovascular problems; or (2) all other reasons — “less likely to be related to psychosocial work factors” — such as musculoskeletal disorders due to surgery or fractures, or mental health diseases (e.g., schizophrenia). The classification of category-1 diagnoses (potentially related to psychosocial work factors) was then refined into eight specific sub-categories (see table 1).
Interviews. During Fall 1997 and 1998, 30-minute telephone interviews were conducted with all active nurses by a specialized firm. Interviewers received training from the research coordinator and interviews were quality-controlled throughout the survey period, in the guise of regular audits performed by the coordinator to ensure questions were posed per instructions and response categories repeated according to prescribed frequency.
The telephone interviews measured current psychosocial factors at work with validated instruments. Psychological demands (quantity of work, intellectual requirements and job time constraints), decision latitude (opportunities to make decisions, be creative, and use and develop one’s abilities at work), and social support at work, from supervisors and colleagues (socio-emotional support or esteem, which is of a socio-psychological or interpersonal nature; instrumental support, which measures extra resources or assistance with work tasks; and a negative level of support, hostility or conflict), were measured using 26 items from Karasek’s Job Content Questionnaire (Karasek, 1985), a widely-used instrument recognized for its sound psychometric properties and French validated version (Brisson et al., 1998). In the second interview only, rewards at work (salary, respect, job security and promotion opportunities) from the ERI model, were measured by Siegrist’s validated instrument (Siegrist, 1996), and the extrinsic efforts component of the model was replaced by psychological demands in this study. Intrinsic effort from Siegrist’s model was also replaced by a surrogate for overinvestment: Type A behaviour which measures individual competitiveness and excessive efficiency at work (Friedman and Rosenman, 1974).
Other variables were measured as potential confounding factors: off-work social support (nature of social network and satisfaction derived) (Santé Québec, 1995); personal and socio-occupational characteristics (age, family status, workplace seniority, job status, work shift, smoking and alcohol consumption).
Data Analysis
Data analysis was performed using SAS 8.2 (SAS Institute Inc., 2000) and SPlus 6.2 (SPlus, 1993) for UNIX. All the analyses were initially done on certified sick leave (CSL) for all diagnoses to test a non-specific effect of psychosocial factors on health (Brisson, Vézina and Vinet, 1985), and then on CSL for mental health problems. The evolution of incidence density (ID) (or incidence rate) and of duration of CSL across restructuring periods was examined. Sub-periods characterizing the timeframe of the health care network restructuring were defined according to major organizational changes that actually occurred during the 6-year follow-up. The five sub-periods were: (i) before restructuring (1993–95); (ii) the anticipation period when the restructuring plan was known but not yet in effect (1995–96); (iii) the major restructuring year (1996–97); (iv) the first year after restructuring (1997–98); and (v) the second year after restructuring (1998–99). Every episode of each nurse’s CSL was recorded along with the number of follow-up days during which the nurse was at risk of absence, i.e. total number of work days in each restructuring period minus total number of days of absence from work for any reason (not only CSL). ID was defined as the total number of CSL episodes for all nurses divided by the total number of follow-up days for all nurses (Rothman and Greenland, 1998). IDs and their 95% confidence interval (CI) were then expressed in 100 person-years. ID was calculated for each previously defined restructuring period. A trend test was performed to estimate and test the ID slope over periods spaced at equal intervals. As subjects may have experienced more than one CSL episode within a given period, or from one period to another, the correlation among these episodes for each period was taken into account when computing the standard error and p-values with the bootstrap method (Efron, 1979). The evolution in CSL total duration by period (sum of days of absence for all CSL episodes beginning in each period, by nurses) was then studied. Generalized Estimating Equations (GEE) (Diggle, Liang and Zeger, 1994) were used to compare total duration means by periods for nurses with at least one CLS in the period. All total durations of the first period (two years) were divided by two to be comparable with the other periods which lasted one year. Linear trends on means were performed using the same procedures as for the ID evolution trend analysis.
The analysis also examined the effect of psychosocial work and other factors on the incidence of certified sick leave over a period of 17 months after the first interview, from November 1997 to March 1999. For each psychosocial work factor, the total score of items was established according to the recommended method (Karasek, 1985). Psychological demands and decision latitude exposures were determined by a threshold at the distribution median of the total score in a comparable population of nurses (11 for psychological demands and 70 for decision latitude) (Bourbonnais et al., 1998). Social support and rewards exposures were determined with a threshold at the distribution median of nurses in this study. The analysis compared a group of exposed nurses to a group of non-exposed nurses for each psychosocial work factor. Four job-strain exposure groups were defined: (i) unexposed or reference group reporting low demands and high latitude; (ii) most exposed group reporting high demands and low latitude; (iii) and (iv) moderately exposed reporting the other two combinations of demands and latitude. Effort/reward imbalance was defined as a ratio of psychological demands on rewards greater than 1. Survival analysis is the appropriate method for this type of data (Kalbfleish and Prentice, 1980). Incidence density ratios (IDR) were used to compare different exposure subgroups of nurses, and to estimate the association between each independent variable and CSL. The Andersen-Gill method for the Cox model was used for multivariate analyses because it allows modeling for time-dependent exposures and multiple events for one subject (Cox and Oakes, 1984). All independent and potentially confounding variables (except rewards and ERI which were measured only in the second interview in 1998), were considered as time-dependent: before mid April 1998, the value in the 1997 interview is applied, and after, the value of the second 1998 interview. For missing data at one interview or the other, the value of the completed interview was kept for the whole follow-up period. The potential modifying effect of social support, rewards and Type A behaviour on job strain and ERI was examined by stratification and, when significant, interaction terms were introduced in the multivariate model. Variables associated with CSL that were also actual confounders of the association between job strain and CSL (change in IDR > 10%), were kept in the final models. Adjusted IDR with their 95% CI are presented. A robust estimator of variance was calculated to take into account inter-subject correlation.
Results
Among 2878 active nurses in September 1997, 276 could not be contacted because of missing or inexact address or telephone number, and 2006/2602 agreed to participate in a telephone interview (77% response rate among those contacted). Among those who retired between April 1995 and September 1997, 274/374 agreed to answer questions related to their health and reasons for leaving the job (73% response rate) (figure 1).
Figure 1
Selection of Participants

* Active nurses not contacted because of missing or inexact data N = 276
Based on available data, participating and non-participating active nurses were comparable according to work shifts (p = 0.95), but were different with respect to job status (p = 0.007): full time nurses responded in a greater proportion than did part time nurses.
Certified sick leave data were compiled from the sick-leave records of 1,454 nurses who had participated in the telephone interview and had given their written consent (1,314 active nurses (66% response rate) and 138 retired nurses (50% response rate)) (figure 1). On the basis of data from the telephone interview, participant and non-participant active nurses were comparable in terms of occupational status, having gone through a change of health care facility or of care unit, prevalence of adverse psychosocial factors on the job (psychological demands, decision latitude, combination of the two, social support) and prevalence of psychological distress. However, there was a lower participation rate among 20–34 year olds (59% compared with 66% of 35–44 year olds and, 68% of 45–60 year olds) (p = 0.0104). The same pattern was true for length of service in the health care facility; nurses who had 21 years or more of service participated more than the others (69% compared to 66% for 12 to 20 years, and 62% for less than 12 years of service (p = 0.0333)). There was no available data for comparison of participants and non-participants among the retired nurses.
Active nurses were predominantly female (94%), and 22–58 years old (mean 42). The vast majority were employed by acute-care facilities (90%), provided direct care (83%), and worked full time (57%). Approximately half worked on day shift (54%), 24% on evening shift, 17% on night shift, and 5% on rotation. Mean length of service in the facility was 17 years. Of the retired participants, most were female (97%), between 30 and 65 years old (mean 55.8), with a mean of 23.4 years of employment in the institution, showing a high level of workplace stability.
The distribution of CSL per type of diagnosis and duration is presented in table 1. Over the 6-year follow-up (1993–99), 52% of the nurses (749/1454) had taken at least one certified sick leave (CSL); 27% had taken one leave, 12% had taken two, 8% had taken three and 5% had taken four or more. Of the total 1,402 spells of CSL, 64.3% (N = 901) were “potentially related to psychosocial work factors.” Among these, mental health problems ranked as the most frequent diagnoses, accounting for 25% of spells and lasting an average of 70 days, followed by musculo-skeletal problems (18%), which lasted 41 days on average.
Sick Leave for All Diagnoses
The evolution of incidence (ID) and of duration of CSL during the five restructuring periods is presented in tables 2–3. For CSL for all diagnoses, there was no statistically significant difference in ID through the periods (table 2), but there was a statistically significant difference in mean number of sick leave days (p < 0.0001, 4 degrees of freedom (df)), which increased significantly (slope of 7.59, test for trend by period, p < 0.0001) (table 3). The mean was lower during the period before restructuring and was higher during the anticipation period and the first year after restructuring (table 3). Then, during the second year after restructuring, it dropped 7.5 days from the preceding period but was still 24 days over the baseline level, before the restructuring. The same pattern is observed with the sum of duration.
Sick Leave for Mental Health Diagnoses
For mental health sick leave, the test for trend in ID increase during the five periods was statistically significant (slope of 1.75, p < 0.0001) (table 2). For the last two periods after restructuring, IDs were statistically higher than during the period before restructuring. There was also a statistically significant difference in mean duration of mental health sick leave by period (p = 0.0018, 4 df) (table 3). The mean increased until the first year after restructuring, and decreased during the second year after restructuring, as was the case for sick leave for all diagnoses, but was also still 24 days over the baseline level. This increase in mean duration was statistically significant (slope of 9.24, test for trend by period, p = 0.0339). The sum number of days of duration was always increasing.
Table 1
Certified Sick Leave Spells by Diagnostic Sub-Categories and Mean Duration among 749 Nurses Who Had at Least One Spell of Sick Leave (1993–1999)

Table 2
Incidence Density (ID) of Sick Leave for All Diagnoses and for Mental Health Problems by Restructuring Periods among 1454 Nurses (1993–1999)
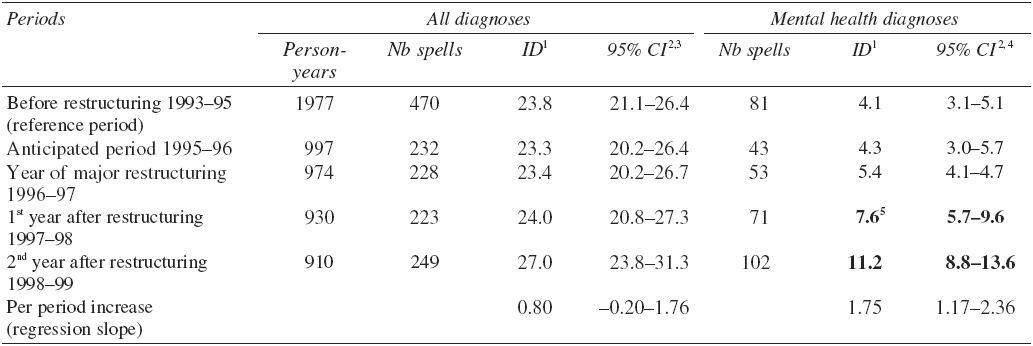
1 ID =incidence density for 100 person-years.
2 Confidence intervals calculated by bootstrap method.
3 Test for trend on the five periods for all diagnoses (p = 0.1126).
4 Test for trend on the five periods for mental health diagnoses (p < 0.0001).
5 The bold font has been used to highlight statistically significant figures comparing to the reference period.
Table 3
Sum and Mean Duration of Sick Leave Spells1 for All Diagnoses and for Mental Health Problems by Restructuring Periods among Nurses Who Had at Least One Spell of Sick Leave (749 Nurses for All Diagnoses and 265 Nurses for Mental Health) (1993–1999)

1 Duration of spells is defined as the sum of days of absence for all CSL episodes beginning in each period.
2 Confidence intervals calculated by bootstrap method.
3 Test for trend on the five periods for all diagnoses (p < 0.0001).
4 Test for trend on the five periods for mental health diagnoses (p = 0.0339).
5 The bold font has been used to highlight statistically significant figures comparing to the reference period.
The effect of psychosocial work factors measured by interview on the 17-month incidence of sick leave for all diagnoses was then examined. Table 4 shows the occupational factors associated with an increased incidence of CSL adjusted for age, occupational status and previous absence: low decision latitude, each combination of job strain, low social support, low rewards, and effort/reward imbalance. Evening (IDR = 1.80; IC: 1.34–2.42), night schedule (IDR = 1.67; IC: 1.17–2.37), off-work social support (IDR = 1.38; IC: 1.06–1.78), age (IDR = 1.02; IC: 1.00–1.03) and regular smoking (IDR = 1.81; IC: 1.36–2.42) were also associated with the incidence of CSL. The following variables were not associated with this type of sick leave: psychological demands, occupational status, job title, type of health care facility and care unit, number of job station changes, type A behaviour, gender, marital status, and alcohol intake.
Table 4
Adjusted1 Incidence Density Ratio (IDR) of Sick Leaves for all Diagnoses by Work Factors among 1314 Active Nurses (1997–1999)

1 IDR adjusted for age, occupational status and previous absence.
2 Job strain: PD = psychological demands; DL = decision latitude; + = high; – = low.
3 Homogeneity test for job strain categories: crude p = 0.0587 and adjusted p = 0.0256.
4 The bold font has been used to highlight statistically significant figures.
The association between CSL for all diagnoses and job strain was free of confounding by other factors, except social support which contributed to a significant change of the association (at least 10% of IDR) when introduced in a multivariate model. The IDR for the combination of high demands and low latitude adjusted for social support, age, occupational status and previous absence was (1.67; IC: 1.07–2.61). Social support at work and Type A behaviour did not modify the association but rewards did (p = 0.0010). The ID ratio was higher among nurses exposed simultaneously to any level of job strain and low rewards. It is noteworthy that nurses in passive jobs (low demands and low latitude) that combined low rewards have the highest risk of sick leave for all diagnoses. The nurses who reported high rewards were no longer at risk of sick leave, whatever the job strain category (table 5).
Table 5
Adjusted1 Incidence Density Ratio (IDR) of Sick Leaves for All Diagnoses by Job Strain and Rewards among 1314 Active Nurses (1997–1999)

1 IDR adjusted for age, occupational status and previous absence.
2 Job strain: PD = psychological demands; DL = decision latitude; + = high; – = low.
3 The bold font has been used to highlight statistically significant figures.
The analysis of sick leaves for a mental health diagnosis adjusted for age, occupational status and previous absence showed significant associations with high psychological demands, the combination of high demands with either high or low latitude, low social support, low rewards, and effort/reward imbalance (table 6). There also was a significant association with age (IDR = 1.03; IC: 1.00–1.06), low off-work social support (IDR = 1.49; IC: 1.01–2.22), and regular smoking (IDR = 1.94; IC: 1.31–2.87). There was no association between mental health sick leave and work status, job title, care unit, schedule, number of job station changes, gender, Type A behaviour or alcohol intake. The association between CSL for a mental health problem and job strain was free of confounding by other factors except social support, as was the association with CSL for all diagnoses. The IDR for the combination of high demands and low latitude adjusted for social support, age, occupational status and previous absence was (2.43; IC: 1.22–4.83). Finally, work social support, Type A behaviour and rewards were not significant modifiers of the association between job strain and sick leave for mental health problems.
Table 6
Adjusted1 Incidence Density Ratio (IDR) of Sick Leaves for Mental Health Problems by Work Factors among 1314 Active Nurses (1997–1999)

1 IDR adjusted for age, occupational status and previous absence.
2 Job strain: PD = psychological demands; DL = decision latitude; + = high; – = low.
3 Homogeneity test for job strain categories : crude p = 0.0491 and adjusted p = 0.0056.
4 The bold font has been used to highlight statistically significant figures.
Discussion
The results showed a non-significant increase of CSL incidence for all diagnoses, but a significant increase in their mean duration across the restructuring periods until the second year after restructuring where it was still 24 days in excess of the baseline level. This is concordant with other studies reporting a negative effect of organizational downsizing on sickness absences (Burke, 2003; Kivimäki et al., 2000). Based on information gathered from interviews, it may be hypothesized that the increased sick leave incidence was nonetheless attenuated by the fact that nurses felt responsible for maintaining the quality of care and did not always take a leave when they were sick (presenteeism). Also, many nurses with less seniority could not spare to lose days, weeks or months of tenure during this period of restructuring when this tenure would allow them to apply for preferred positions in the hospital. In addition, they may have resorted to authorized absences other than sick leave that did not impact seniority (return to school for specialization, leave without pay, leave with differed remuneration). However, this pressure to attend may have exacerbated health problems, which would be consistent with an increase in sick leave duration during the restructuring periods (Bourbonnais et al., 1992).
As for sick leave for mental health problems, there was a significant increase in incidence density across the restructuring periods, and an important increase in the duration of CSL. The trend was homogeneous throughout the six acute care facilities (88% of the total sample size). Sample sizes for the remaining seven non-acute care institutions were too small to assess homogeneity of this trend within these smaller facilities. These results agree with interview data showing a greater prevalence of psychological distress and psychotropic drug use among these nurses during the restructuring period in comparison with a representative provincial sample of working women in 1998 (Bourbonnais et al., 2005). No other empirical study has documented sick leave for mental health problems during major restructuring. However, our results are consistent with data reported in 2001 by a provincial committee on income insurance for sick leave which showed an increase in the ratio of hours paid in income insurance (for mental health and for all diagnoses) divided by hours worked by the healthcare personnel since 1993 (Ministère de la Santé et des Services sociaux, 2001b).
Our results showed a significant effect of low decision latitude and every combination of demands on the incidence of certified sick leave for all diagnoses. Although the effect of high psychological demands was in the right direction, it was not statistically significant. This is concordant with results from a study within a French national electricity and gas company where low levels of decision latitude were associated with more frequent and longer sickness absences for both men and women, but high psychological demands were not for women (Niedhammer et al., 1998).
Our results also show a moderating effect of rewards on the association between job strain and the incidence of sick leave for all diagnoses. Nurses who reported high rewards were no longer at risk of sick leave, whatever the job strain category. Although this moderating effect of rewards has not been previously documented, a few studies have reported an association between effort-reward imbalance (ERI) and burnout among nurses (Bakker et al., 2000), psychiatric morbidity in a cohort of civil servants (Stansfeld et al., 1999), emotional exhaustion, psychosomatic complaints and physical symptoms in employees in various job sectors (De Jonge et al., 2000), and an independent association between effort-reward imbalance/low control at work and depression in a small electric equipment production plant (Tsutsumi et al., 2001). Godin and Kittel (2004) found an association between high level of ERI and self-reported absenteeism in different firms, after adjusting for the economic stability of these firms. Peter and Siegrist (1997) found low reward to be associated with short-term and long-term sickness absence and number of spells (company’s registered) among middle managers whereas no indicator of high effort at work was associated with sickness absence. Furthermore, De Jonge et al. (2000) showed an independent, cumulative effect of job strain and effort reward imbalance on well-being. Because the measure of extrinsic efforts in this study was substituted by psychological demands which is also part of the job strain measure, the cumulative effect of job strain and ERI could not be tested.
High psychological demands were associated with certified sick leave for mental health problems and this is concordant with results from the Whitehall II study, which was conducted among London civil servants and showed an effect of psychological demands on the incidence of short spells of sick leave for psychiatric disorders (North et al., 1996) among women (Stansfeld, Fuhrer et al., 1997).
Low social support at work was associated with an increased incidence of sick leave for all diagnoses and for mental health problems. Similar results were observed in the Whitehall II study for short absences due to mental health problems in men and women, and for long absence due to mental health problems in women but not in men (Stansfeld, Rael et al., 1997). However, social support did not modify the effect of job strain on the incidence of sick leave for all diagnoses nor for mental health problems in our study. Only Parkes, Mendham and von Rabenau (1994) observed a significant moderating effect of social support on the association between job strain and somatic symptoms among health-care workers.
Strengths of the Study
This study has several strengths, including a longitudinal design that enables examination of certified sick leave over a 6-year follow-up period covering different restructuring phases and the use of objective data for measuring sick leaves. Using certified sick leave extracted from valid employee records diminished the possibility of an information bias. Each medical certificate was issued by a treating physician who was not employed by the health care facility. Thus, although the treating physician is not necessarily immune to his patient’s wishes, he would not have any incentive for interpreting the patient’s symptoms as work-related since such an interpretation is not required for insurance compensation. In fact, medical certificates rarely indicate a work-related disease since occupational risk factors are not routinely investigated by general practitioners. In addition, it is to note that the increase seen in ID for mental health diagnoses cannot be attributed to a shift over time in the way medical practitioners attributed the diagnoses (from other reasons to mental health reasons) since the increase in ID is also seen for all diagnoses. The characterization of certified sick leave for mental health problems “potentially related to psychosocial work factors” allowed a precise classification of outcomes. In addition, the validity of the outcome measure is supported by previous studies (Marmot et al., 1995), (Bourbonnais and Mondor, 2001), which showed an association between mental health indicators at baseline and subsequent certified sick leave, especially related to mental health.
Interview data made it possible to evaluate the effect of specific psychosocial work factors on certified sick leave, while controlling for known potential confounders as well as less-documented ones, including off-work factors as recommended by Johns et al. (1997) in their review of contemporary research on work absence.
Limitations of the Study
The study also has some weaknesses, particularly its lack of a control group, which was unavailable since the restructuring was carried out in all health facilities province-wide. Overall, the lack of a control group makes it impossible to verify whether the increased sick leave is due to restructuring or is simply part of a generalized phenomenon affecting various occupational sectors, which may or may not be undergoing major transformation or downsizing. However, an increase in psychosocial work factors during the restructuring was documented among nurses and these constraints are associated with sick leave among nurses (Bourbonnais et al., 2005).
Selection bias is a potential limitation as only 66% of active nurses and 50% of retired nurses agreed to participate in the 6-year follow-up of sick leave. However, active nurses who agreed to participate were comparable to non-participating nurses for all occupational factors and for the prevalence of psychological distress. This is consistent with unbiased participation. Selection bias may also have occurred if the mass retirements in July 1997 allowed those planning to take sick leave to retire, thus leaving nurses in better health at work and reducing a possible increase in sick leave among non-retirees. Indeed, in 1993–95, before the restructuring, retired nurses showed a higher sick leave incidence density, than active nurses (IDR = 1.32 (1.02–1.73). Therefore, since ID was quite high among active nurses after 1997, it is conceivable that it would have been even higher if the retired nurses had not left.
A possible selection bias pertains to the healthy worker effect (HWE) if sick nurses got out of the workforce either by retirement or sick leave and did not participate in the study. This bias would entail an underestimation of the incidence of sick leaves. We have diminished this kind of bias in choosing the telephone interview which reached all active nurses, including nurses who were temporarily out of work. In fact, seven percent of respondents reported that they had been absent from work for a prolonged period at the time of interview, and this was due to sickness for only 3 %. We also carried out a short telephone interview among 274 of the 374 nurses who had left their employment since the beginning of restructuring, between April 1995 and September 1997 (73% response rate). From an open question pertaining to the main reason which had motivated them to leave their job, 13% left because of physical and/or emotional exhaustion, and 7% for other health problems. Another selection bias may have occurred if nurses who participated in the telephone survey were not representative of all the nurses eligible for the study. This bias would have entailed either an over or underestimation of the prevalence of either health problems or work psychosocial factors. However, we achieved a good participation rate, therefore minimizing the possibility and the magnitude of this selection bias. The comparison of respondents and non-respondents revealed that fewer part-time nurses participated in the study. This lower participation remains difficult to explain and the direction of the effect is unknown.
Information bias related to the self-reported measure of exposure is a potential directional bias in the results of the effect of specific psychosocial work factors. However, no objective measure of the nurses’ work within each care unit was available. Moreover, external assessments may lack important information regarding psychosocial factors (North et al., 1996) and it seems likely the effects of working conditions on future mental health are mediated by individual perceptions of work. Thus, susceptibility to psychiatric disorders related to work cannot be separated from one’s personal perceptions and reactions to working conditions (Stansfeld et al., 1999).
Conclusion
The present study adds to previous findings showing an increase in the incidence and duration of sick leave among nurses during a major restructuring period. This is particularly true for leaves related to mental health. These results support the idea that important changes in the work environment should be carefully planned to prevent the deterioration of psychosocial factors which have been documented to have an impact on employees’ health and their sickness absence. This is in line with Vinet who proposes orientations to favour healthy and productive workplaces which include: the integration of health concerns and goals at the very beginning of an organizational change and the pursuit of preventive intervention (Vinet, 2004: 335–380).
The present study identified adverse work psychosocial factors associated with CSL which are modifiable and provide some basis for preventive interventions. Indeed, it was reported that the elevated levels of psychological distress among nurses exposed to job strain returned to levels observed among nurses who have never been exposed to job strain, when the exposure was removed (Bourbonnais, Comeau and Vézina, 1999). Moreover, many studies have demonstrated that an improvement in the psychosocial work conditions such as an increase in job control during transformation and downsizing, reduces the risk of sick leave among workers (Bond and Bunce, 2001; Kivimäki et al., 2000; Parker, Chmiel and Wall, 1997; Vahtera et al., 2000).
Since human resources are the mainstay and primary resource of the health network, it is essential that people be able to carry out their work under optimal conditions. In this line, a ministerial committee report proposes a rethinking of the overall work organization taking into account factors of presence at work and bolstering the esteem of health-care personnel (Ministère de la Santé et des Services sociaux, 2001a). In a recent conference on mental health at work, a representant of the Québec Labour ministry mentioned that health, and specifically mental health, is a major focus for the government and, the best way to insure it is to act on factors that contribute more to the development of a healthy workplace which respects individuals and factors on which organizations are able to intervene efficiently (Audet et al., 2003: 61). This could be achieved by stabilizing work teams (thus reducing psychological demands and increasing social support), giving all personnel more responsibilities, allowing them to participate in decision-making (more latitude), fostering coordination through exchanges, discussions and inter-team communication (more social support), encouraging local initiatives, promoting expertise transfer and proposing mechanisms for acknowledging the personnel’s work, and mechanisms oriented towards the development of individual and team abilities (more rewards).
As outlined by many authors during the 58th congress of the Industrial Relations Department of Laval University, organizational factors which offer the best guarantee of mental health are: a work organization which can strike a balance between work demands and decision latitude; work conditions that allows better regulation of modern life contingencies; managers who favour transparency in communications, who listen to their employees and are able to detect emerging conflicts and manage them; and an organizational culture which values the respect of individuals, recognizes their contribution, avoids excessive competition and invests in its human capital in the long term (Audet et al., 2003).
Finally, as Brun underlines at the same congress, in the field of prevention, a great number of levers are present in the organizations and if mental health problems are of psychological nature, solutions are not only psychological and lie also in existing management practices. It is a matter not of introducing new practices but of improving usual ones (Brun, 2003).
Parties annexes
Acknowledgement
This study received financial support from the Québec Ministry of Health and Social Services, the Québec Social Research Council and the Canadian National Health Research Development Program. We wish to acknowledge the collaboration of all nurses, advisory committee members, human resources managers and union representatives who participated to the research in each health care facility. We also wish to thank Mélanie Lavoie-Tremblay for supervising the collection of sick leave data, as well as Myrto Mondor and Marc Simard for their data processing efforts, Richard Whelan and Ursula Donovan for reviewing the English version of this paper.
References
- Audet, M., J.-P. Brun, C. Blais, S. Montreuil, and A. Vinet. 2003. Santé mentale et travail: l’urgence de penser autrement l’organisation. Québec: Les Presses de l’Université Laval.
- Bakker, A. B., C. H. Killmer, J. Siegrist, and W. B. Schaufeli. 2000. “Effort-Reward Imbalance and Burnout among Nurses.” Journal of Advanced Nursing, 31 (4), 884–891.
- Bond, F. W., and D. Bunce. 2001. “Job Control Mediates Change in a Work Reorganization Intervention for Stress Reduction.” Journal of Occupational Health Psychology, 6 (4), 290–302.
- Bosma, H., M. G. Marmot, H. Hemingway., A. C. Nicholson, E. Brunner, and S. A. Stansfeld. 1997. “Low Job Control and Risk of Coronary Heart Disease in Whitehall II (prospective cohort) Study.” British Medical Journal, 314 (7080), 558–565.
- Bourbonnais, R., C. Brisson, R. Malenfant, and M. Vézina. 2005. “Health Care Restructuring, Work Environment, and Health of Nurses.” American Journal of Industrial Medicine, 47 (1), 54–64.
- Bourbonnais, R., M. Comeau, G. Dion, and M. Vézina. 1998. “Job Strain, Psychological Distress, and Burnout in Nurses.” American Journal of Industrial Medicine, 34 (1), 20–28.
- Bourbonnais, R., M. Comeau, and M. Vézina. 1999. “Job Strain and Evolution of Mental Health among Nurses.” Journal of Occupational Health Psychology, 4 (2), 95–107.
- Bourbonnais, R., and M. Mondor. 2001. “Job Strain and Sickness Absence among Nurses in the Province of Québec.” American Journal of Industrial Medicine, 39 (2), 194–202.
- Bourbonnais, R., and M. Vézina. 1995. “La santé mentale des cols blancs et l’environnement psychosocial du travail.” Santé Mentale au Québec, XX (2), 163–184.
- Bourbonnais, R., and A. Vinet. 1989. “L’absence du travail comme indicateur de santé: signification, mesures et conditions d’utilisation.” Revue d’Épidémiologie et de Santé Publique, 37, 173–182.
- Bourbonnais, R., A. Vinet, M. Vézina, and S. Gingras. 1992. “Certified Sick Leave as a Non Specific Morbidity Indicator: A Case-Referent Study among Nurses.” British Journal of Industrial Medicine, 49, 673–678.
- Brisson, C., C. Blanchette., C. Guimont, G. Dion, J. Moisan, M. Vézina, et al. 1998. “Reliability and Validity of the French Version of the 18-item Karasek Job Content Questionnaire.” Work & Stress, 12 (4), 322–336.
- Brisson, C., M. Vézina, and A. Vinet. 1985. “Organisation du travail et santé mentale: le travail répétitif sous contrainte de temps.” Santé Mentale au Québec, X, 13–30.
- Brun, J.-P. 2003. “Miser sur les pratiques de gestion comme outil de prévention en santé mentale au travail.” Santé mentale et travail: l’urgence de penser autrement l’organisation. M. Audet et al., eds. Québec: Les Presses de l’Université Laval, 143–158.
- Burke, R. J. 2003. “Survivors and Victims of Hospital Restructuring and Downsizing: Who are the Real Victims?” International Journal of Nursing Studies, 40, 903–909.
- Cox, D. R., and D. Oakes. 1984. Analysis of Survival Data. London: Chapman and Hall.
- De Jonge, J., H. Bosma, R. Peter and J. Siegrist. 2000. “Job Strain, Effort-Reward Imbalance and Employee Well-Being: A Large Scale Cross-Sectional Study.” Social Science & Medicine, 50 (9), 1317–1327.
- Diggle, P. J., K. Y. Liang, and S. L. Zeger. 1994. Analysis of Longitudinal Data. Oxford, U.K.: Oxford University Press.
- Efron, B. 1979. “Bootstrap methods: another look at the Jacknife.” Annals of Statistics, 7, 1–26.
- Friedman, M., and R. Rosenman. 1974. Type A Behavior and Your Heart. New York: Knopf.
- Gerpott, T. J. 1990. “Intracompany Job Transfers: An Exploratory Two-Sample Study of the Buffering Effects of Interpersonal Support.” Prevention in Human Services, 8 (1), 113–137.
- Godin, I., and F. Kittel. 2004. “Differential Economic Stability and Psychosocial Stress at Work: Associations with Psychosomatic Complaints and Absenteeism.” Social Science & Medicine, 58 (8), 1543–1553.
- Greenglass, E. R., R. J. Burke and L. Fiksenbaum. 2001. “Workload and Burnout in Nurses.” Journal of Community and Applied Social Psychology, 11, 211–215.
- Greenglass, E. R., R. J. Burke, and L. Fiksenbaum. 2002. “Impact of Restructuring, Job Insecurity and Job Satisfaction in Hospital Nurses.” Stress News, 14 (1).
- Harrison, D. A., and J. J.Martocchio. 1998. “Time for Absenteeism: A 20–Year Review of Origins, Offshoots, and Outcomes.” Journal of Management, 24 (3), 305–350.
- Johns, G. 1997. “Contemporary Research on Absence from Work: Correlates, Causes and Consequences.” International Review of Industrial and Organizational Psychology, 12, 115–173.
- Johnson, J. V., E. M. Hall, and T. Theorell. 1989. “Combined Effects of Job Strain and Social Isolation on Cardiovascular Disease, Morbidity and Mortality in a Random Sample of the Swedish Male Working Population.” Scandinavian Journal of Work, Environment & Health, 15, 271–279.
- Kalbfleish, J. D., and R. L. Prentice. 1980. The Statistical Analysis of Failure Time Data. New York: Wiley.
- Karasek, R. 1985. Job Content Questionnaire and User’s Guide. Los Angeles: Department of Industrial and System Engineering, University of Southern California.
- Karasek, R., and T. Theorell. 1990. Healthy Work: Stress, Productivity and the Reconstruction of Working Life. New York: Basic Books.
- Karttunen, A. 1995. All Worked Up, Work Health Safety 1995. Helsinki, Finland: Institute of Occupational Health.
- Kivimäki, M., J. Head., J. E. Ferrie, M. J. Shipley, J. Vahtera, and M. G. Marmot. 2003. “Sickness Absence as a Global Measure of Health: Evidence from Mortality in the Whitehall II Prospective Cohort Study.” British Medical Journal, 327 (7411), 364–374.
- Kivimäki, M., J. Vahtera, J. Pentti, and J. E. Ferrie. 2000. “Factors Underlying the Effect of Organizational Downsizing on Health of Employees: Longitudinal Cohort Study.” British Medical Journal, 320 (7240), 971–975.
- Marmot, M., A. Feeney, M. Shipley, F. North, and S. L. Syme. 1995. “Sickness Absence as a Measure of Health Status and Functioning: From the UK Whitehall II Study.” Journal of Epidemiology and Community Health, 49 (2), 124–130.
- Matteson, M. T., and J. M. Ivancevich. 1990. “Merger and Acquisition Stress: Fear and Uncertainty at Mid-Career.” Prevention in Human Services, 8 (1), 139-158.
- Ministère de la Santé et des Services sociaux. 2001a. Rapport du Comité provincial d’assurance salaire. Plan d’action ministériel à l’égard de la présence au travail 2001–2004. Québec: Gouvernement du Québec.
- Ministère de la Santé et des Services sociaux. 2001b. Rapport du comité provincial d’assurance salaire. Plan d’action ministériel à l’égard de la gestion de la présence au travail. Québec: Gouvernement du Québec.
- Niedhammer, I., I. Bugel, M. Goldberg, A. Leclerc, and A. Guéguen. 1998. “Psychosocial Factors at Work and Sickness Absence in the Gazel Cohort: A Prospective Study.” Occupational and Environmental Medicine, 55 (11), 735–741.
- North, F. M., L. Syme, A. Feeney, M. Shipley, and M. G. Marmot. 1996. “Psychosocial Work Environment and Sickness Absence among British Civil Servants: The Whitehall II Study.” American Journal of Public Health, 86 (3), 332–340.
- Parker, S. K., N. Chmiel, and T. D. Wall. 1997. “Work Characteristics and Employee Well-Being within a Context of Strategic Downsizing.” Journal of Occupational Health Psychology, 2 (4), 289–303.
- Parkes, K. R., C. A. Mendham, and C. von Rabenau. 1994. “Social Support and the Demand-Discretion Model of Job Stress: Tests of Additive and Interactive Effects in Two Samples.” Journal of Vocational Behavior, 44 (1), 91–113.
- Peter, R., and J. Siegrist. 1997. “Chronic Work Stress, Sickness Absence, and Hypertension in Middle Managers: General or Specific Sociological Explanations?” Social Science & Medicine, 45 (7), 1111–1120.
- Rothman, K. J., and S. Greenland. 1998. Modern Epidemiology. 2nd ed. Philadelphia: Lippincott-Raven.
- Santé Québec, C. Bellerose, C. Lavallée, L. Chénard, and M. Levasseur. 1995. Et la santé, ça va en 1992–93? Rapport de l’enquête sociale et de santé 1992-1993. Vol. 1. Montréal: Ministère de la Santé et des Services sociaux, Gouvernement du Québec.
- SAS Institute Inc. 2000. The SAS System for Sun OS. Cary, North Carolina: SAS Institute.
- Sauter, S. L., L. R. Murphy, and J. J. Hurrell. 1990. “Prevention of Work-Related Psychological Disorders: A National Strategy Proposed by the National Institute for Occupational Safety and Health (NIOSH).” American Psychologist, 45 (10), 1146–1158.
- Schaufeli, W. B., and M. A. J. Kompier. 2001. “Managing Job Stress in the Netherlands.” International Journal of Stress Management, 8 (1), 15–34.
- Siegrist, J. 1996. “Adverse Health Effects of High-Effort/Low-Reward Conditions.” Journal of Occupational Health Psychology, 1 (1), 27–41.
- SPlus. 1993. Programmer’s Manual. Seattle: StatSci, MathSoft.
- Stansfeld, S. A., R. Fuhrer, J. Head, J. Ferrie and M. Shipley. 1997. “Work and Psychiatric Disorder in the Whitehall II Study.” Journal of Psychosomatic Research, 43 (1), 73–81.
- Stansfeld, S. A., R. Fuhrer, M. J. Shipley, and M. G. Marmot. 1999. “Work Characteristics Predict Psychiatric Disorder: Prospective Results from the Whitehall II Study.” Occupational and Environmental Medicine, 56 (5), 302–307.
- Stansfeld, S. A., E. G. S. Rael, J. Head, M. Shipley, and M. Marmot. 1997. “Social Support and Psychiatric Sickness Absence: A Prospective Study of British Civil Servants.” Psychological Medicine, 27, 35–48.
- Tsutsumi, A., K. Kayaba, T. Theorell, and J. Siegrist. 2001. “Association between Job Stress and Depression among Japanese Employees Threatened by Job Loss in a Comparison between Two Complementary Job-Stress Models.” Scandinavian Journal of Work, Environment & Health, 27 (2), 146–153.
- Vahtera, J., M. Kivimäki, P. Pentti, and T. Theorell. 2000. “Effect of Change in the Psychosocial Work Environment on Sickness Absence: A Seven Years Follow Up of Initially Healthy Employees.” Journal of Epidemiology and Community Health, 54 (7), 484–493.
- van der Doef, M., and S. Maes. 1999. “The Job Demand-Control (-Support) Model and Psychological Well-Being: A Review of 20 Years of Empirical Research.” Work & Stress, 13 (2), 87–114.
- Vézina, M. 1998. “La santé mentale au travail. Peut-il y avoir place à la lésion professionnelle?” Le Médecin du Québec, 33 (4), 113–116.
- Vézina, M., M. Cousineau, D. Mergler, A. Vinet, and M. C. Laurendeau. 1992. Pour donner un sens au travail. Bilan et orientations du Québec en santé mentale au travail. Boucherville: Gaëtan Morin.
- Vinet, A. 2004. Travail, organisation et santé. Le défi de la productivité dans le respect des personnes. Sainte-Foy, Québec: Les Presses de l’Université Laval.
- Woodward, C. A., H. S. Shannon, B. Lendrum, J. Brown, J. McIntosh, and C. Cunningham. 2000. “Predictors of Job Stress and Satisfaction among Hospital Workers during Re-Engineering: Differences by Extent of Supervisory Responsibilities.” Healthcare Management FORUM Gestion des soins de santé, 13 (1), 29–35.
- Xie, J. L., and J. Schaubroeck. 2001. “Bridging Approaches and Findings across Diverse Disciplines to Improve Job Stress Research.” Research in Occupational Stress and Well Being Volume 1: Exploring Theoretical Mechanisms and Perspectives. P. L. Perrewe and D. C. Ganster, eds. Oxford: Elsevier Science, 1–61.
Liste des figures
Figure 1
Selection of Participants
* Active nurses not contacted because of missing or inexact data N = 276
Liste des tableaux
Table 1
Certified Sick Leave Spells by Diagnostic Sub-Categories and Mean Duration among 749 Nurses Who Had at Least One Spell of Sick Leave (1993–1999)
Table 2
Incidence Density (ID) of Sick Leave for All Diagnoses and for Mental Health Problems by Restructuring Periods among 1454 Nurses (1993–1999)
1 ID =incidence density for 100 person-years.
2 Confidence intervals calculated by bootstrap method.
3 Test for trend on the five periods for all diagnoses (p = 0.1126).
4 Test for trend on the five periods for mental health diagnoses (p < 0.0001).
5 The bold font has been used to highlight statistically significant figures comparing to the reference period.
Table 3
Sum and Mean Duration of Sick Leave Spells1 for All Diagnoses and for Mental Health Problems by Restructuring Periods among Nurses Who Had at Least One Spell of Sick Leave (749 Nurses for All Diagnoses and 265 Nurses for Mental Health) (1993–1999)
1 Duration of spells is defined as the sum of days of absence for all CSL episodes beginning in each period.
2 Confidence intervals calculated by bootstrap method.
3 Test for trend on the five periods for all diagnoses (p < 0.0001).
4 Test for trend on the five periods for mental health diagnoses (p = 0.0339).
5 The bold font has been used to highlight statistically significant figures comparing to the reference period.
Table 4
Adjusted1 Incidence Density Ratio (IDR) of Sick Leaves for all Diagnoses by Work Factors among 1314 Active Nurses (1997–1999)
1 IDR adjusted for age, occupational status and previous absence.
2 Job strain: PD = psychological demands; DL = decision latitude; + = high; – = low.
3 Homogeneity test for job strain categories: crude p = 0.0587 and adjusted p = 0.0256.
4 The bold font has been used to highlight statistically significant figures.
Table 5
Adjusted1 Incidence Density Ratio (IDR) of Sick Leaves for All Diagnoses by Job Strain and Rewards among 1314 Active Nurses (1997–1999)
1 IDR adjusted for age, occupational status and previous absence.
2 Job strain: PD = psychological demands; DL = decision latitude; + = high; – = low.
3 The bold font has been used to highlight statistically significant figures.
Table 6
Adjusted1 Incidence Density Ratio (IDR) of Sick Leaves for Mental Health Problems by Work Factors among 1314 Active Nurses (1997–1999)
1 IDR adjusted for age, occupational status and previous absence.
2 Job strain: PD = psychological demands; DL = decision latitude; + = high; – = low.
3 Homogeneity test for job strain categories : crude p = 0.0491 and adjusted p = 0.0056.
4 The bold font has been used to highlight statistically significant figures.